
Peer Reviewed
Progressive Confusion and Recurrent Falls After Bariatric Surgery
Answer: C Wernicke encephalopathy
Nonalcoholic Wernicke encephalopathy is characterized by acute or chronic thiamine (vitaminB1) deficiency. Thiamine is a key cofactor in several enzymatic steps involved in energy metabolism and is especially important during periods of high metabolic demands such as during the postoperative period where metabolism can increase as much as 15% to 30%.1,2 More importantly, thiamine stores in the liver last up to 18 days and rapidly deplete in malnourished patients.1 The classic triad of ataxia, changes in mental status, and ophthalmoplegia are seen only in a subset of patients, making early clinical diagnosis challenging.3
Differential diagnosis
Nonalcoholic Wernicke encephalopathy presents less commonly in adult and pediatric patient populations, secondary to bariatric surgery, chronic dietary deficiency, anorexia nervosa, hyperemesis gravidarum, gastrointestinal tumors, prolonged fasting, prolonged parental nutrition, acquired immunodeficiency syndrome, and chemotherapy.3-5 Bariatric surgery patients, particularly those who have had Roux-en-Y gastric bypass or biliopancreatic diversion with duodenal switch, are highly susceptible to thiamine deficiency due to the rerouting of their alimentary tract, which bypasses the duodenum and proximal jejunum where the majority of vitaminB1 is absorbed. Wernicke encephalopathy can occur after bariatric surgery within the immediate postoperative period (as soon as 3 weeks); however, the risk may be lifelong in the presence of other risk factors, including infections, insufficient meals, and alcohol consumption.6 Mortality is as high as 20%, with severe, permanent neurological deficits despite thiamine replacement.7Diagnostic testing
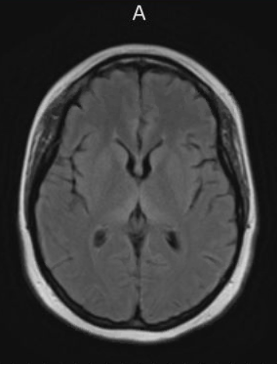
Workup should include measuring a serum thiamine level in addition to a magnetic resonance imaging (MRI) of the brain with and without contrast with concurrent neurology consultation. MRI will traditionally show T2 hyperintense signal abnormalities involving the bilateral posterior medial thalami symmetrically with increased signal in the periaqueductal area and tectal plate (Figure). Signal abnormalities in the mamillary bodies may present but are less common.3,4
Treatment and management
Treatment of nonalcoholic Wernicke encephalopathy is thiamine 500 mg IV 3 times daily for 3 days, followed by 250 mg IV daily for 5 days, and then 100 mg by mouth daily thereafter. Folate acid 1 mg should be added. Intravenous “banana bags” containing nutritive additives that include mutivitamins with vitamin K, magnesium sulfate, thiamine, and folic acid are commonly administered in infusions centers and hospitals, but intramuscular injections have been administered in office settings as well. Thiamine should be given liberally as thiamine is nontoxic, even at high levels.8,9 It is important to note that solutions containing glucose should not be administered before replenishing thiamine stores as it can precipitate Korsakoff syndrome.8Patient outcome
The patient’s serum thiamine level was 70. The findings of an MRI were consistent with Wernicke’s encephalopathy. The patient was hospitalized for 8 days with IV thiamine repletion and subsequently discharged on a daily oral thiamine regimen. At discharge, the patient showed significant improvement in her neurologic function, with mild fine motor deficits and steady gait. Repeat MRI prior to discharge showed improvement in signal abnormalities. In this case, the patient was fortunate in that she showed remarkable recovery. Vitamin repletion does not always reverse the clinical deficits.Learning points
Given the ever-growing prevalence of morbid obesity and the concordant rise of bariatric surgeries, nonalcoholic Wernicke encephalopathy associated with bariatric surgery should be considered as a cause of Wernicke encephalopathy. In addition, there is an increase in litigation related to this entity.8 Establishing thiamine deficiency is not readily available and serum levels may not accurately reflect brain thiamine levels. Improved clinical and radiographic recognition can lead to earlier diagnosis, and prompt treatment improves the likelihood of reversal and full neurologic recovery. Therefore, high clinical suspicion and awareness among physicians is key for optimal patient outcomes.AUTHORS:
Christopher J. Lundberg, DO1 • Daniel Tran, DO2 • Alan Lucerna, DO3 • James Espinosa, MD3 • Eric Maddock, DO3 • Robin J. Lahr, DO3AFFILIATIONS:
1Department of Emergency Medicine, FirstHealth of the Carolinas, Pinehurst, NC
2Department of Cardiology, Rowan University School of Osteopathic Medicine, Stratford/Jefferson Health New Jersey, Stratford, NJ
3Department of Emergency Medicine, Jefferson Health New Jersey, Stratford, NJCITATION:
Lundberg CJ, Tran D, Lucerna A, Espinosa J, Maddock E, Lahr RJ. Progressive confusion and recurrent falls after bariatric surgery. Consultant. 2022;62(12):e5. doi:10.25270/con.2022.02.00011Received September 11, 2021. Accepted October 20, 2021. Published online May 23, 2022
DISCLOSURES:
The authors report no relevant financial relationships.CORRESPONDENCE:
Alan Lucerna, DO, Department of Emergency Medicine, Jefferson Health New Jersey, 18 East Laurel Road, Stratford, NJ 08084 (Alan.Lucerna@jefferson.edu)
1. Osiezagha K, Ali S, Freeman C, et al. Thiamine deficiency and delirium. Innov Clin Neurosci. 2013;10(4):26-32.
2. Şimşek T, Şimşek HU, Cantürk NZ. Response to trauma and metabolic changes: post-traumatic metabolism. Ulus Cerrahi Derg. 2014;30(3):153-159. doi:10.5152/UCD.2014.2653
3. Santos Andrade C, Tavares Lucato L, da Graca Morais Martin M, et al. Br J Radiol. 2010;83(989):437-446. doi:10.1259/bjr/27226205
4. Lyons DA, Linscott LL, Krueger DA. Non-alcoholic Wernicke encephalopathy. Pediatr Neurol. 2016;56:94-95. doi:10.1016/j.pediatrneurol.2015.12.007
5. Busani S, Bonvecchio C, Gaspari A, et al. Wernicke’s encephalopathy in a malnourished surgical patient: a difficult diagnosis. BMC Res Notes. 2014;7:718. doi:10.1186/1756-0500-7-718
6. Oudman E, Wijnia JW, van Dam M, Biter LU, Postma A. Preventing Wernicke encephalopathy after bariatric surgery. Obes Surg. 2018;28(7):2060-2068. doi:10.1007/s11695-018-3262-4
7. Aasheim ET. Wernicke encephalopathy after bariatric surgery: a systematic review. Ann Surg. 2008;248(5):714-720. doi:10.1097/SLA.0b013e3181884308
8. DeMaria E, Trigilio-Black C. Alarming increase in malpractice claims related to Wernicke’s encephalopathy post bariatric surgery: an alert to monitor for thiamine deficiency. Bariatric Times. 2018;15(7):8-9.
9. Dung D, Chien K, Ma L. Case report: Wernicke encephalopathy following Roux-en-Y gastric bypass. Am Fam Physician. 2020;102(4):197-198.