
Peer Reviewed
How Would You Diagnose This Neonate’s Abnormal Head Shape?
Correct answer: E. Craniosynostosis
The differential diagnosis for cranial deformities in neonates includes molding secondary to fetal head constraint in the birth canal, plagiocephaly, microcephaly, and torticollis among others. For our patient, a second ultrasonography scan of the head revealed a partial metopic craniosynostosis. A computed tomography (CT) scan with 3-dimensional reconstruction of the head and face was performed and confirmed the diagnosis of craniosynostosis of the metopic suture (Figure 3).
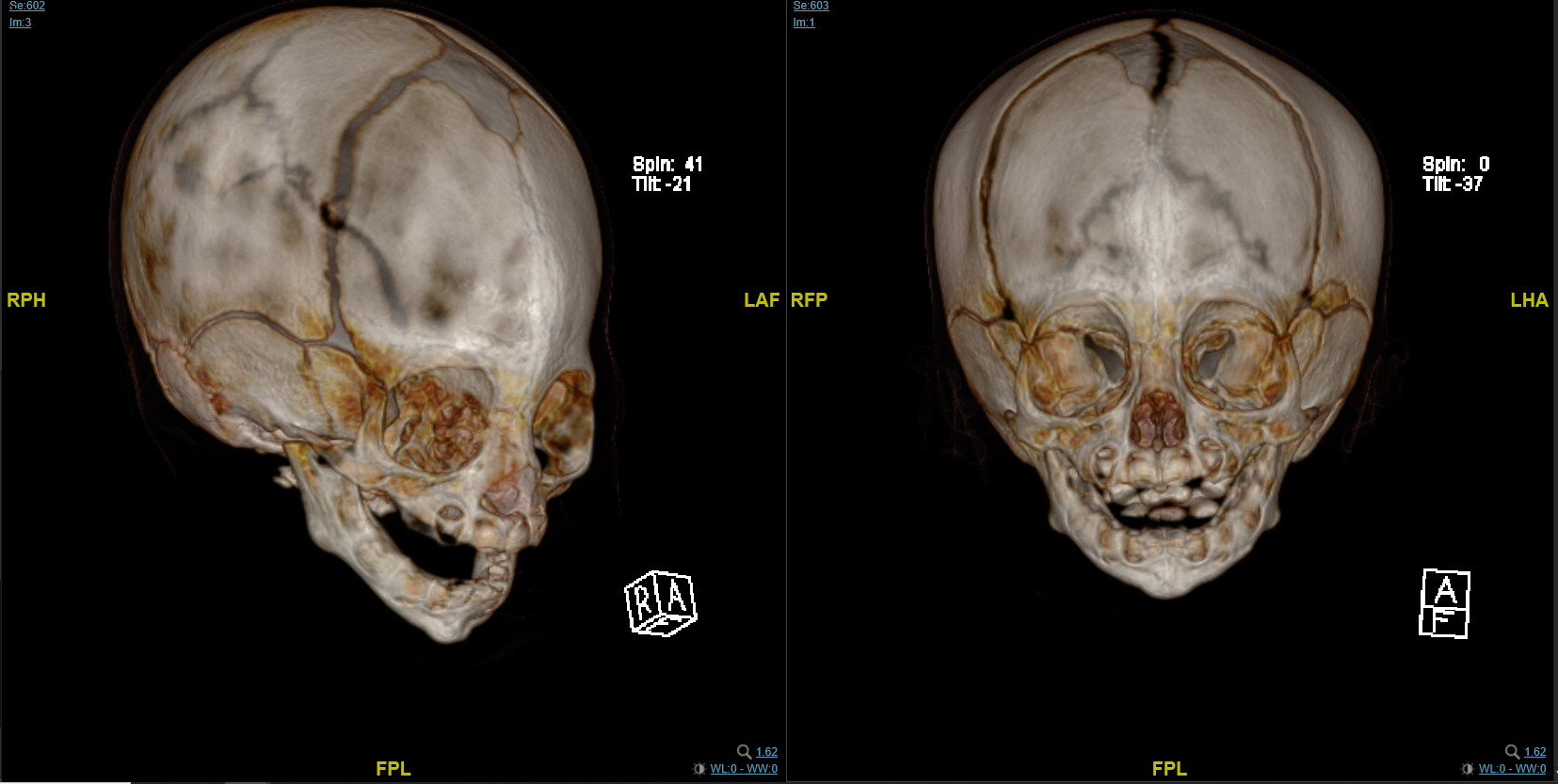
Figure 3. A computed tomography scan with 3-dimensional reconstruction of the head and face confirmed the diagnosis of craniosynostosis of the metopic suture.Cephalometrics were not performed on our patient. Although this study does have a role in craniosynostosis and is high yield for a low cost, it is limited by the complexity of the craniofacial form and operator dependence in choosing the landmarks measured.1
Discussion. Separation, via sutures, of the cranial vault bones is essential during infancy to allow adequate passage through the birth canal, as well as to permit growth of the skull during brain development. Craniosynostosis is defined clinically as a premature union of the cranial sutures. Craniosynostosis can be classified into primary (an intrinsic defect of ossification) or secondary (occurring as part of systemic disease). They can be categorized as simple (one suture involved) or complex (multiple sutures involved). Craniosynostosis can be an isolated finding (nonsyndromic) or part of a larger group of symptoms (syndromic).
Metopic synostosis accounts for about 15% of cases of craniosynostosis.2 This synostosis is the second-most common form of craniosynostosis. The metopic suture is one of the first sutures to close on the calvarium.3 Some reports cite closure as early as age 3 months and as late as age 9 months.3,4 Premature closure results in trigonocephaly, a term derived from the Greek words "trigonon" (triangle) and "kephale" (head). Hermann Welcker was the first to use this term in 1862 to describe wedge-shaped skulls.3 The incidence of metopic craniosynostosis has been on the rise over the past several decades, with a currently reported incidence of 1:700 to 1:15,000 live births and a predominance in boys.3
Several etiologies have been proposed for the occurrence of metopic synostosis. The most common of these is an intrinsic bone malformation, where ossification occurs early in the pregnancy because of genetic causes (eg, Apert syndrome), metabolic causes (eg, hypothyroidism), or pharmacotherapy (eg, valproic acid use).3,4 The second-most common proposed etiology is a fetal head constraint, which is seen in a later phase of pregnancy (secondary to multiparous pregnancies, oligohydramnios, or head constraint in the pelvic area).2,3
Of all the single suture synostosis cases, children with metopic synostosis have a higher correlation with neuropsychological developmental problems.3 Most of these become apparent when children reach school age, given increasing complexity of school demands and social interactions. Speech and reading are not as affected, although patients do have a higher risk of learning disabilities.2
The diagnosis of most types of craniosynostosis can be made clinically. It is important to perform a thorough physical examination to determine not only the head circumference and skull shape but also to make note of size, shape, and tensions of all fontanelles. As noted above, craniosynostosis can be syndromic or nonsyndromic. As such, physical examinations should also note the presence of any dysmorphic features or congenital anomalies. A thorough prenatal history should be obtained to determine risk factors such as intrauterine constraint, abnormal fetal head position, and drug use during pregnancy, as well as the presence of oligohydramnios.
However, there is a role for radiologic imaging in the diagnosis of craniosynostosis, particularly when minor sutures are involved or when the patency of sutures is difficult to assess.5 Currently, the standard of care is a clinical examination followed by a cranial ultrasonography scan. Cranial ultrasonography scans are beneficial because they are radiation-free and can be performed rapidly without the need for sedation.5 The provider performing the scan can visualize and examine the head, which aids in correlating the ultrasonography scan with physical examination findings.6 That said, ultrasonography scans are limited by operator dependence. In their study, Katya Rozovsky and colleagues found that metopic synostosis was a challenge to diagnose via conventional radiography and cranial ultrasonography scans, given such early closure of the suture.6
CT scans of the brain with 3-dimensional reconstruction remains the gold standard for diagnosing craniosynostosis. Not only can it assess suture lines adequately, but it can also evaluate for additional brain abnormalities and aid in future surgical planning.5 For metopic synostosis, CT scans may show hypotelorism, hypoplastic ethmoid sinus, a medially upward-slanted orbital roof (also known as the "quizzical eye"), and a narrow anterior cranial fossa.5,7 While a CT scan with 3-dimensional reconstruction is useful for obtaining a definitive diagnosis, the Working Group of Craniosynostosis guidelines still recommend an initial radiography or cranial ultrasonography scanning as first-line diagnostic tools.8 This is due to less exposure to radiation, particularly for patients younger than 1 year of age. The scans can be repeated in 1 to 2 months in indeterminate cases, particularly in very young infants.
Magnetic resonance imaging (MRI) has also been studied as an alternative for diagnosing craniosynostosis. However, this imaging modality is not without its risks to the patient. While it eliminates radiation risks, it also requires the patient to be completely still, which incurs the need for sedation or general anesthesia. Additionally, the scans do not show suture lines as well as a CT scan, although protocols are in development to increase appreciation of sutures lines with the use of an MRI.2,5
Treatment and management. The current treatment for craniosynostosis is geared toward achieving normal brain development by creating sufficient space for brain growth. Consequences of untreated craniosynostosis may include abnormal head shape, developmental delay, and increased intracranial pressure.2,4 Fundoscopic evaluation of increased intracranial hypertension is found in less than 2% of patients with metopic craniosynostosis, making it a rare complication.4 It should also be noted that craniosynostosis can occur as part of genetic syndromes, and as such, some of these complications may be due to the syndrome more than the skull abnormality alone.4
Interventions for craniosynostosis can range from remodeling helmets alone to surgery or a combination of both. Referral to a craniofacial team after diagnosis can help guide this decision. The optimal age for surgical management is still debated but is usually between 6 and 12 months of age.2 Surgical modalities include an endoscopic procedure or an open craniotomy with reconstruction. Multiple factors determine which surgical modality is appropriate for each patient. In general, endoscopic surgeries are preferred for children younger than 6 months of age, since the cranial bones are still flexible enough to be manipulated. Endoscopic surgeries often have a faster postoperative recovery period, but most patients require remolding helmets after surgery.2 Open craniotomy and reconstruction are better for complex suture repairs, syndromic craniosynostosis, or operations performed in patients older than 6 months of age (given stiffness of bones). While it comes with the risks associated with any major surgical procedure, open craniotomy does allow for better outcomes when a lot of remodeling is required.2
In general, an endoscopic approach incurs fewer complications than an open craniotomy. In both surgical approaches, the most common postoperative complication is hyperthermia.2 Other complications include meningitis, wound infection, postoperative hematomas (ie, subgaleal, subdural), dural tear, cerebrospinal fluid leak, and intraoperative bleeding.2 The postoperative mortality rate is 2.6%, and postoperative morbidity rate is 12%.2
Patient outcome. Once the diagnosis was made, our patient was referred to a neurosurgeon and a plastic surgeon. At 3 months of age, our patient underwent an endoscopic strip craniectomy of the metopic suture. After the surgery, a remodeling helmet was used until 12 months of age. A geneticist also evaluated the patient, considering the hypospadias and umbilical hernia, for concern of syndromic craniosynostosis. The most common genetic causes for syndromic craniosynostosis are microdeletion/duplications, which were ruled out in our patient with a normal microarray.
Other single-gene disorders, like X-linked or autosomal-dominant opitz G/BBB, were considered, but ultimately our patient did not fit the characteristic features of any of these syndromes. The decision was made to hold further genetic testing unless developmental delay or new medical concerns develop. At 5 months of age, the patient developed gross motor delays, which were eventually resolved after early intervention. At his last follow-up, the patient was 20 months of age. He was growing adequately and meeting developmental milestones as expected for age (Figure 4). He has no other major medical issues.

Figure 4. The patient’s craniosynostosis resolved after surgery. This gross image shows him a few months postoperatively.References
1. McIntyre GT, Mossey PA. Size and shape measurement in contemporary cephalometrics. Eur J Orthod. 2003;25(3):231-242. https://doi.org/10.1093/ejo/25.3.231
2. Kajdic N, Spazzapan P, Velnar T. Craniosynostosis - Recognition, clinical characteristics, and treatment. Bosn J Basic Med Sci. 2018;18(2):110-116. https://doi.org/10.17305/bjbms.2017.2083
3. van der Meulen J. Metopic synostosis. Childs Nerv Syst. 2012;28(9):1359-1367. https://doi.org/10.1007/s00381-012-1803-z
4. Vinchon M. The metopic suture: natural history. Neurochirurgie. 2019;65(5):239-245. https://doi.org/10.1016/j.neuchi.2019.09.006
5. Massimi L, Bianchi F, Frassanito P, Calandrelli R, Tamburrini G, Caldarelli M. Imaging in craniosynostosis: when and what? Childs Nerv Syst. 2019;35(11):2055-2069. https://doi.org/10.1007/s00381-019-04278-x
6. Rozovsky K, Udjus K, Wilson N, Barrowman NJ, Simanovsky N, Miller E. Cranial ultrasound as a first-line imaging examination for craniosynostosis. Pediatrics. 2016;137(2):e20152230. https://doi.org/10.1542/peds.2015-2230
7. Kim HJ, Roh HG, Lee IW. Craniosynostosis: updates in radiologic diagnosis. J Korean Neurosurg Soc. 2016;59(3):219-226. https://doi.org/10.3340/jkns.2016.59.3.219
8. Mathijssen IMJ. Guideline for care of patients with the diagnoses of craniosynostosis: Working Group on Craniosynostosis. J Craniofac Surg. 2015;26(6):1735-1807. https://dx.doi.org/10.1097%2FSCS.0000000000002016