
Peer Reviewed
A Nonhealing Ulcer With Secondary Enlarging Nodules in a Linear Distribution
Answer: Nodular Lymphangitis (Sporotrichoid Spread)
Test results for Histoplasma, Blastomyces, and Coccidioides antibodies were negative, and results of an interferon-γ release assay were negative for Mycobacterium tuberculosis. Two punch biopsies were performed, the findings of which were significant for focal abscesses within the epidermis and granulomas within the dermis. Tissue stains and cultures were found to be negative for acid-fast bacilli (AFB). Fungal culture of the tissue was positive for Paecilomyces species, a ubiquitous organism and frequent contaminant. Bacterial culture of one of the tissue samples was positive for Staphylococcus epidermidis, which was interpreted as a likely contaminant. Bacterial culture of the second tissue sample was positive for Staphylococcus aureus.
The patient was subsequently diagnosed with nodular lymphangitis, suspected to be secondary to S aureus infection. He was prescribed minocycline, 100 mg twice daily for 28 days.
On a follow-up visit 3 months later, the patient had had near complete resolution of the skin lesions with residual scarring.
DISCUSSION
Nodular lymphangitis, commonly known as sporotrichoid spread, is the progressive development of cutaneous nodules along the dermal and subcutaneous lymphatic vessels in a linear distribution.1 The distinct pattern radiates from the primary lesion, which often presents as a firm erythematous nodule that is prone to ulceration.2,3
The differential diagnosis of nodular lymphangitis includes cutaneous sarcoidosis, cutaneous tumor metastasis, cat-scratch disease, and cellulitis. The similarities between these conditions are notable in the physical examination findings, but certain features of nodular lymphangitis make it distinct.
Cutaneous sarcoidosis can present without systemic symptoms but does not display the distal-to-proximal development of linear nodules. The more defining lesions of cutaneous sarcoidosis are clustered papules or plaques,4 which were not seen in this patient.
Cutaneous tumor metastasis would be less likely in a 19-year-old person with lesions that are not characteristic in appearance for a primary cutaneous tumor, such as melanoma. Histopathological examination would assuredly rule out a primary cutaneous tumor in this case.5
Cat-scratch disease is often accompanied by systemic symptoms of fever, headache, or fatigue and presents with regional nodular lymphadenopathy rather than linear lymphadenopathy. The patient in this case had had no recent exposure to cats, decreasing the likelihood of Bartonella henselae inoculation.6,7
Cellulitis can present with ascending lymphangitis. The patient in this case had developed the primary lesion a year prior, which had maintained a stable surface area without treatment. Cellulitis would be expected not only to increase in the surface area of the primary site, but also to present as exceptionally tender. A patient with cellulitis for a year’s duration would likely have experienced systemic symptoms.8
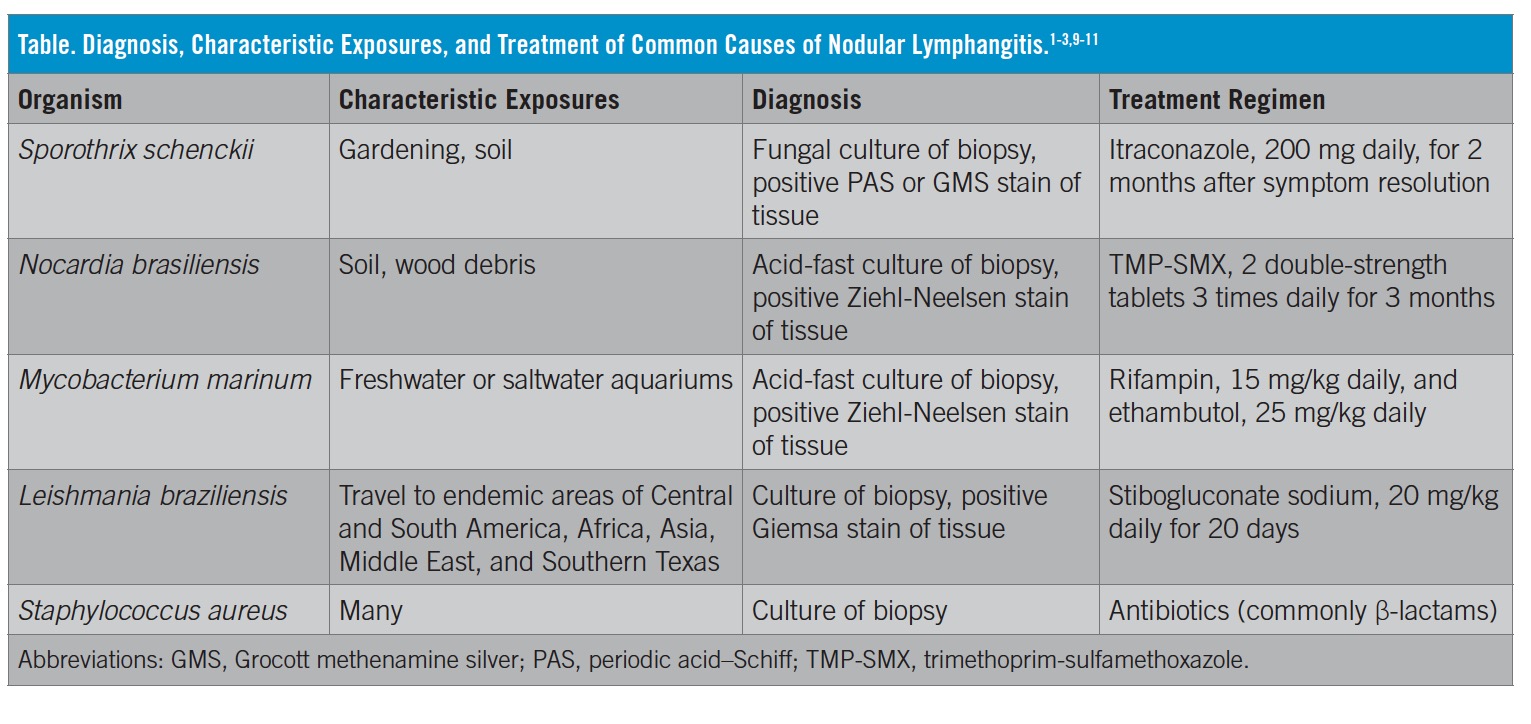
The diagnosis of nodular lymphangitis is often made based on its characteristic appearance and then confirmed with identification of the infectious agent. Common causative agents of nodular lymphangitis include Sporothrix schenckii, Nocardia brasiliensis, Mycobacterium marinum, Leishmania braziliensis and S aureus, although many others have been described. In order to determine the causative organism and the treatment approach, a number of procedures should be performed. Based on clinical suspicion, exposures, and geographical region, these procedures may include a tissue biopsy, special stains for fungus and AFB, fungal cultures, AFB cultures, and bacterial cultures of the tissue. Histopathology results without stain will likely be nonspecific, with granuloma and abscess identification in most of the common etiologies.1-3
The accompanying Table offers a brief summary of characteristic features for organisms that are commonly associated with nodular lymphangitis and their treatment regimens.
REFERENCES:
- Tobin EH, Jih WW. Sporotrichoid lymphocutaneous infections: etiology, diagnosis and therapy. Am Fam Physician. 2001;63(2):326-332.
- Heller HM, Swartz MN. Nodular lymphangitis: clinical features, differential diagnosis and management. Curr Clin Top Infect Dis. 1994;14:142-158.
- Tirado-Sánchez A, Bonifaz A. Nodular lymphangitis (sporotrichoid lymphocutaneous infections). Clues to differential diagnosis. J Fungi (Basel). 2018;4(2):56. doi:10.3390/jof4020056
- Katta R. Cutaneous sarcoidosis: a dermatologic masquerader. Am Fam Physician. 2002;65(8):1581-1584.
- Filosa A, Filosa G. Melanoma diagnosis: the importance of histopathological report. Dermatopathology (Basel). 2018;5(1):41-43. doi:10.1159/000486670
- Carithers HA. Cat-scratch disease: an overview based on a study of 1,200 patients. Am J Dis Child. 1985;139(11):1124-1133. doi:10.1001/archpedi.1985.02140130062031
- Maman E, Bickels J, Ephros M, et al. Musculoskeletal manifestations of cat scratch disease. Clin Infect Dis. 2007;45(12):1535-1540. doi:10.1086/523587
- Nichols RL, Florman S. Clinical presentations of soft-tissue infections and surgical site infections. Clin Infect Dis. 2001;33(suppl 2):S84-S93. doi:10.1086/321862
- Wright NA, Davis LE, Aftergut KS, Parrish CA, Cockerell CJ. Cutaneous leishmaniasis in Texas: a northern spread of endemic areas. J Am Acad Dermatol. 2008;58(4):650-652. doi:10.1016/j.jaad.2007.11.008
- Edelstein H. Mycobacterium marinum skin infections: report of 31 cases and review of the literature. Arch Intern Med. 1994;154(12):1359-1364. doi:10.1001/archinte.1994.00420120079009
- Saubolle MA, Sussland D. Nocardiosis: review of clinical and laboratory experience. J Clin Microbiol. 2003;41(10):4497-4501. doi:10.1128/jcm.41.10.4497-4501.2003