
Peer Reviewed
Bilateral Developmental Dysplasia of the Hip
Authors:
Alexander Wetzig, BS; Fatima Aly, MD; and Lynnette Mazur, MD
McGovern Medical School at the University of Texas Health Science Center at Houston
Citation:
Wetzig A, Aly F, Mazur L. Bilateral developmental dysplasia of the hip. Consultant. 2018;58(9):256-257.
A 12-year-old girl presented to with left-sided hip pain and a limp that had been progressively worsening over the past 8 months. Although she was a soccer player, she denied any history of trauma. She had begun limiting her participation because of the pain.
Physical examination. She had full passive range of motion of her hips joints without subluxation, audible crepitus, or laxity. There was no tenderness to palpation over the bony prominences of the greater trochanters, but she had a positive impingement sign on the left, elicited by hip flexion with internal rotation.
Diagnostic tests. Radiographs showed abnormal lateral center edge angles, which are the angles formed by a vertical line through the center of the femoral head and a line from the center of the femoral head to the lateral edge of the acetabulum; less than 20° is abnormal.1,2 The angles measured -5° on the left and +10° on the right, with poor coverage of the femoral heads and acetabula, worse on the left (Figure 1).

Based on these findings, she received a diagnosis of bilateral developmental dysplasia of the hip (DDH).
Discussion. Previously known as congenital dislocation of the hip, the condition’s name was changed to DDH in 1994 to more accurately reflect that while dysplasia may be detected at birth, it may also develop during infancy or childhood.3 DDH encompasses abnormal development of the acetabulum and proximal femur that results in mechanical instability of the hip joint. In contrast to the teratologic dysplasia associated with conditions such as Ehlers-Danlos syndrome or Down syndrome, or the neuromuscular dysplasia that occurs in patients with spina bifida or cerebral palsy, typical DDH arises in otherwise healthy infants. The prevalence rate is approximately 0.5%. Risk factors include female sex, breech position, a positive family history, and swaddling of the lower extremities.4,5
Embryologically, the hip is completely formed by the 11th week of gestation, and normal development relies on correct anatomic contact promoting mutual induction.6 When physiologic ligamentous laxity is combined with external mechanical forces, eccentric joint contact can lead to an everted and flattened labrum and a shallow acetabulum.6,7 Persistent dysplastic changes lead to decreased anterior and lateral coverage of the femoral head.6 Physical findings for asymmetric DDH in infants include a positive Galeazzi sign or functional femoral shortening, uneven gluteal or thigh skin creases, and limitation of hip abduction to less than 45°. Screening with the Ortolani maneuver, abduction of the hip with simultaneous lifting of the greater trochanter anteriorly, can help with the diagnosis; a palpable “clunk” is felt. The term click is deceptive, because clicks often represent benign ligamentous or tendinous snapping that do not suggest DDH.5 It has been proposed that repetitive forceful Barlow maneuvers can damage the joint and increase the likelihood of instability.8 Screening for DDH in infants is recommended at birth and at every routine visit until the child is walking.5
The natural history of DDH depends on the severity of the dysplasia. In a cohort of nearly 12,000 neonates, 60% of those who screened positive for instability on physical examination had stability restored within the first week of life, and nearly 90% were stable by 2 months.9 For this reason, referral for further imaging and evaluation is made at 2 months of life. Infants and young children rarely have pain or other limitations, and a dislocated hip may function tolerably for many years. One study showed that the time to diagnosis ranged from 3 to 16 years.10 Although the complication rate may be low, over time there is progressive pain and functional disability and accelerated degenerative joint disease.10,11 Unilateral dislocations are at risk for leg-length discrepancies, ipsilateral knee pain, scoliosis, and antalgic gait. Patients with bilateral dislocation may have back pain, and patients with persistent dysplasia without dislocations may develop activity-related pain and premature joint disease in adolescence or young adulthood.1,10-12
Dysplasia diagnosed in adolescence or early adulthood is corrected with surgery.1 Most patients achieve radiologic improvement and improved Harris hip scores, a 10-item scoring system that includes pain, function, absence of deformity, and range of motion. The complications of surgery—avascular necrosis (2% to 3%), loss of fixation (1% to 6%), and pelvic nonunion (4%)—while rare must be balanced with the benefits of improved function and delay in joint degeneration.1,13,14
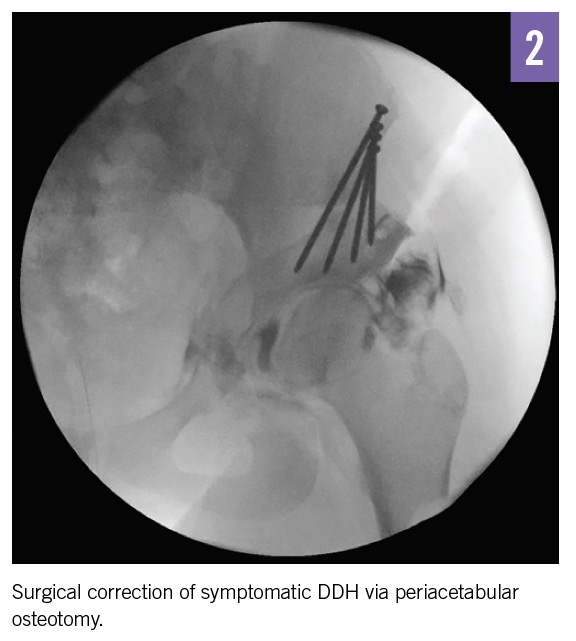
Outcome of the case. After the risks of nonsurgical management were discussed, our patient, her family, and her surgeon agreed on surgical correction with a periacetabular osteotomy (Figure 2). The patient asked when she could return to playing soccer and was told that return to play was reported in 80% of female patients at a median of 9 months after surgery.15
REFERENCES:
- Clohisy JC, Barrett SE, Gordon JE, Delgado ED, Schoenecker PL. Periacetabular osteotomy for the treatment of severe acetabular dysplasia. J Bone Joint Surg Am. 2005;87(2):254-259.
- Petersen BD, Wolf B, Lambert JR, et al. Lateral acetabular labral length is inversely related to acetabular coverage as measured by lateral center edge angle of Wiberg. J Hip Preserv Surg. 2016;3(3):190-196.
- Aronsson DD, Goldberg MJ, Kling TF Jr, Roy DR. Developmental dysplasia of the hip. Pediatrics. 1994;94(2 pt 1):201-208.
- Bialik V, Bialik GM, Blazer S, Sujov P, Wiener F, Berant M. Developmental dysplasia of the hip: a new approach to incidence. Pediatrics. 1999;103(1):93-99.
- Shipman SA, Helfand M, Moyer VA, Yawn BP. Screening for developmental dysplasia of the hip: a systematic literature review for the US Preventive Services Task Force. Pediatrics. 2006;117(3):e557-e576.
- Rális Z, McKibbin B. Changes in shape of the human hip joint during its development and their relation to its stability. J Bone Joint Surg Br. 1973;55(4):780-785.
- Dunn PM. The anatomy and pathology of congenital dislocation of the hip. Clin Orthop Relat Res. 1976;(119):23-27.
- Jones DA. Neonatal hip stability and the Barlow test: a study in stillborn babies. J Bone Joint Surg Br. 1991;73(2):216-218.
- Barlow TG. Early diagnosis and treatment of congenital dislocation of the hip. Proc R Soc Med. 1963;56:804-806.
- Crawford AH, Mehlman CT, Slovek RW. The fate of untreated developmental dislocation of the hip: long-term follow-up of eleven patients. J Pediatr Orthop. 1999;19(5):641-644.
- Wedge JH, Wasylenko MJ. The natural history of congenital dislocation of the hip: a critical review. Clin Orthop Relat Res. 1978;(137):154-162.
- Pun S. Hip dysplasia in the young adult caused by residual childhood and adolescent-onset dysplasia. Curr Rev Musculoskelet Med. 2016;9(4):427-434.
- Terjesen T. Residual hip dysplasia as a risk factor for osteoarthritis in 45 years follow-up of late-detected hip dislocation. J Child Orthop. 2011;5(6):425-431.
- Clohisy JC, Schutz AL, St. John L, Schoenecker PL, Wright RW. Periacetabular osteotomy: a systematic literature review. Clin Orthop Relat Res. 2009;467(8):2041-2052.
- Heyworth BE, Novais EN, Murray K, et al. Return to play after periacetabular osteotomy for treatment of acetabular dysplasia in adolescent and young adult athletes. Am J Sports Med. 2016;44(6):1573-1581.