
Pearls of Wisdom: Premature Ejaculation
Question: Marvin is a 32-year-old man who has been married for 3 years and is planning to start a family. He has experienced premature ejaculation since adolescence and although his partner is willing to “put up with it,” she is not very happy about it. Duration of intercourse is generally less than 1 minute, and he sometimes ejaculates ante portas (ejaculation prior to intromission), which causes himself some embarrassment, his wife some disappointment, and obviously is unsatisfactory in their quest to get pregnant.
He has tried topical lidocaine jelly, but this results in generalized penile numbness. Unless he uses a barrier (thereby compromising pregnancy possibilities), the lidocaine also decreases his wife’s sensitivity.
Marvin says he is willing to try anything that will help his problem, but is really looking for something that will work quickly. He has no current or past major health problems, takes no medications, does not smoke or use illicit substances, and considers himself happily married.
Which message about treatment is appropriate for Marvin?
- Simply distracting himself and thinking about things other than sexuality should be sufficient to manage his premature ejaculation.
- Low dose chronic oral opioids will be helpful.
- SSRIs (e,g, paroxetine) are usually helpful.
- Tricyclic antidepressants (eg, amitryptilene) are usually helpful.
What is the correct answer?
(Answer and discussion on next page)
Louis Kuritzky. MD, has been involved in medical education since the 1970s. Drawing upon years of clinical experience, he has crafted each year for almost 3 decades a collection of items that are often underappreciated by clinicians, yet important for patients. His “Pearls of Wisdom” as we like to call them, have been shared with primary care physicians annually in an educational presentation entitled 5TIWIKLY (“5 Things I Wish I Knew Last Year”…. or the grammatically correct, “5 Things I Wish I’d Known Last Year”).
Now, for the first time, Dr Kuritzky is sharing with the Consultant360 audience. Sign up today to receive new advice each week.
Answer: SSRIs (e,g, paroxetine) are usually helpful.
Clinicians are often surprised to learn that premature ejaculation is one of the most common sexual dysfunctions in men. Their surprise stems from the fact premature ejaculation is not an often-mentioned complaint in the office.
Prevalence of Premature Ejaculation1

The reasons for this are several-fold:
- First, in contrast to the situation with erectile dysfunction (ED), there has been no media blitz that “normalizes” premature ejaculation. In the late 1990s, I have been told that the commercial word Viagra was second only to Coca-Cola in name recognition.
- Second, ED has been “legitimized” as a medical disorder, being typically secondary to endothelial dysfunction associated with hypertension, dyslipidemia, diabetes, and aging. Hence, when one has ED, one is a victim; when one has premature ejaculation—since it is generally recognized to be psychogenic in origin—one is the culprit!
- Third, there are no approved pharmacologic agents to treat premature ejaculation. So, even though premature ejaculation is epidemiologically more prevalent, most men afflicted with the disorder do not seek help for it. This is similar to the situation in the pre-Viagra era when more than 90% of men with ED did not discuss it with their physician, based upon the premise that there was little to be done about it. While it remains true that in mid-life men (age 50 and older), ED is the more common sexual dysfunction, the lifetime prevalence of premature ejaculation places it on parity with ED.
Premature Ejaculation: Definition2

Distraction and Counseling Techniques
Men with premature ejaculation have often tried distraction techniques and topical anesthetics, but are often disappointed with the results. The counseling techniques of Masters and Johnson achieved a very high success rate (>95%), which corroborated the prevailing opinion that premature ejaculation is a psychogenic disorder, or at least it is generally remediable with counseling intervention. Unfortunately, the expense and time commitment required to comply with a Masters and Johnson-type counseling curriculum is beyond the reach of many patients, and they would like something less expensive and more expedient.
When men enter clinical trials for premature ejaculation, their vaginal ejaculatory latency time is generally <1 minute. (Vaginal ejaculatory latency time is the amount of time after insertion of the penis into the vagina until ejaculation occurs).
Premature Ejaculation Rx: SSRIs3,4
SSRIs
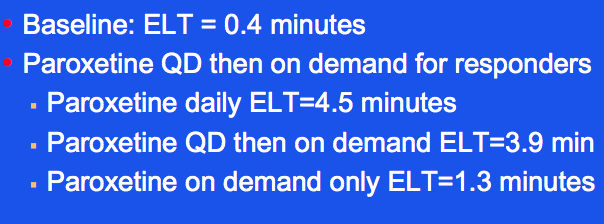
The most recent data on treatments for premature ejaculation capitalizes on the observation that a common adverse effect of SSRIs is delay in ejaculation. For instance, in a study of men who had a baseline ejaculatory latency time of 24 seconds, paroxetine 20 mg either daily for 4 weeks or on demand (administered 3-4 hours before intercourse).
SSRI Sustained Rx Regimen3,4

They found that daily paroxetine increased ejaculatory latency time to 4.5 minutes, compared to only 1.3 minutes for on-demand paroxetine. Interestingly, patients who first used daily paroxetine 20 mg/d and were then switched to on-demand paroxetine still enjoyed a marked improvement in ejaculatory latency time (3.9 minutes).
SSRI Sequential Rx Regimen3,4

Constricting Ring
Other interventions can be helpful for premature ejaculation. For instance, application of a constricting ring—as is supplied with vacuum constriction devices for ED—will maintain turgidity of the penis even after ejaculation, allowing intercourse to continue, if desired.
With a penile constriction band in place, once the patient knows that he can still maintain a substantial degree of turgidity after ejaculation, the reduced anxiety results in lesser production of sympathetic amines associated with detumescence. Hence, the reduction in anxiety allows better maintenance of erection.
Doctor-Patient Interaction
Simply asking a patient how his sex life is will likely result in an anticipated response of “fine.” Instead, consider asking a question to delve a little further.
I suggest: “How would you rate your sex life on a scale of 1-10?”
Most persons will still answer with a number (say 7) and you can follow-up with, “Well, that’s good. What would have to be different to change it from a 7 to a 10?”
The response here is how you can learn about problems like dyspareunia, premature ejaculation, hypoactive sexual desire disorder, etc.
Two algorithms (sustained and on-demand) are provided for consideration.
Note: Utilization of SSRIs for premature ejaculation is an off-label use.
What’s the “Take Home”?
Premature ejaculation has a compelling epidemiologic presence, yet is uncommonly encountered in the office practice setting of primary care clinicians. A comprehensive sexual history should include not only clarity about the ability to obtain a satisfactory erection, but also the ability to maintain it. Patients who are bothered with premature ejaculation often find that SSRI treatment improves their sexual function to a much more satisfactory level.
- Koyuncu H, Serefoglu EC, Yencilek E, et al. Escitalopram treatment for premature ejaculation has a negative effect on semen parameters. Int J Impot Research. 2011;23:257-261.
- Kuritzky L, Samraj G, Seftel A. Premature ejaculation. Patient Care. 2005;39(1):49-54.
- McMahon CG, Touma K. Treatment of rapid ejaculation with paroxetine hydrochloride. Int J Impot Res. 1999;11:241-245.
- McMahon CG, Touma K. Treatment of premature ejaculation with paroxetine hydrcholride as needed: 2 single-blind placebo controlled crossover studies. J Urol. 1999:161:1826-1830.