Pearls of Wisdom: Migraine Medications
Answer: Consider nadolol, because it is likely to be more effective.
Migraine treatment can be at the same time extraordinarily challenging as well as equally rewarding. This is because patients, who are most commonly female, present with a series of failed attempts with medications that are ineffectual to prevent their headaches, inadequate to abort their headaches, are associated with frequent recurrences, or burdened by poorly tolerated adverse effects, including cost.
Fortunately, the diversity of treatment regimens available should encourage clinicians (and their patients) to take heart in the fact that most patients can find a treatment that provides both satisfactory headache relief and is reasonably tolerable. For this discussion, we are focusing upon migraine prophylaxis.
Research
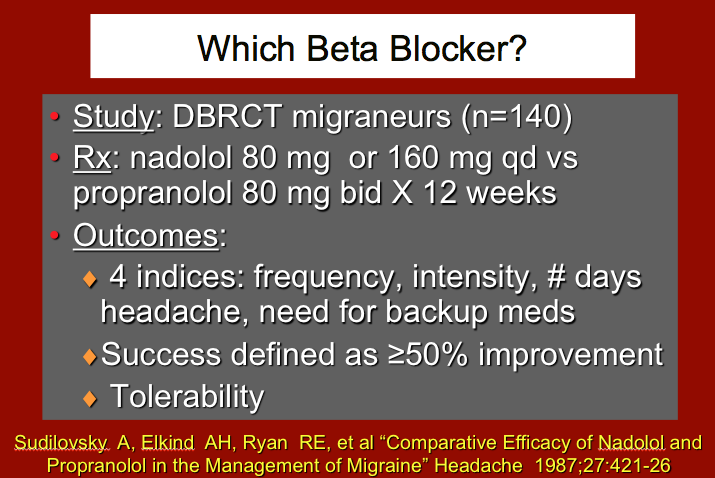
In the study, a “headache score” is used to measure success.1 There is a certain merit and sensibility to the headache score, since it is a composite of the most important clinical endpoints we typically seek: did we favorably affect headache frequency, headache intensity, the absolute number of days with headache, and the number of occasions on which backup medication (for recurrence or insufficient initial relief) was needed.
On the other hand, such a score can also “hide clinical sins.” That is, what if a patient was suffering migraine headaches 3 times a week (total of 12 per month), with an intensity of 6 on an 11-point Likert scale, and 36 total number headache days. Let’s say we provide her a prophylaxis medication (beta blocker, for instance) that reduces her headaches down from 12 headaches to 4 (one weekly, or a 4-fold reduction). That would greatly improve the headache score, wouldn’t it?
But, if at the same time, the headache intensity increased from a 6 to a 9 on an 11-point Likert scale, the patient would very likely be a quite unhappy camper even though her headache score would have been improved dramatically by the 4-fold reduction in headache frequency.

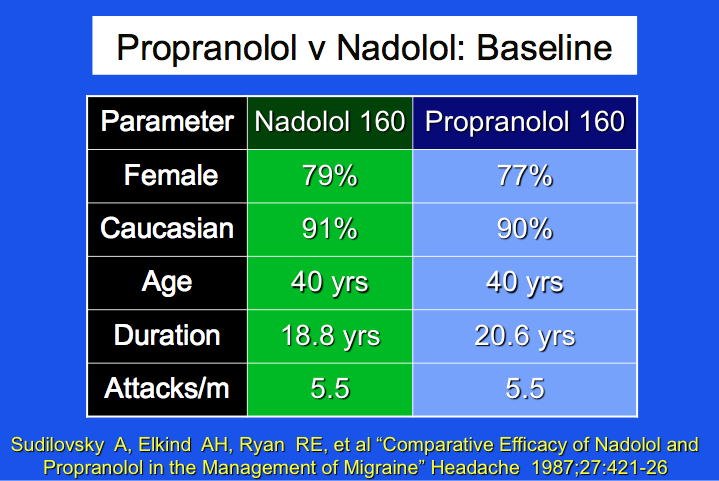
The reason to focus upon the individual components of—as well as the composite score for—the headache index is well illustrated by this oldie-but-goodie double blind randomized clinical trial (DBRCT) comparing equal doses of propranolol (previous trade name Inderal, now generic) and nadolol (previous trade name Corgard, now generic).
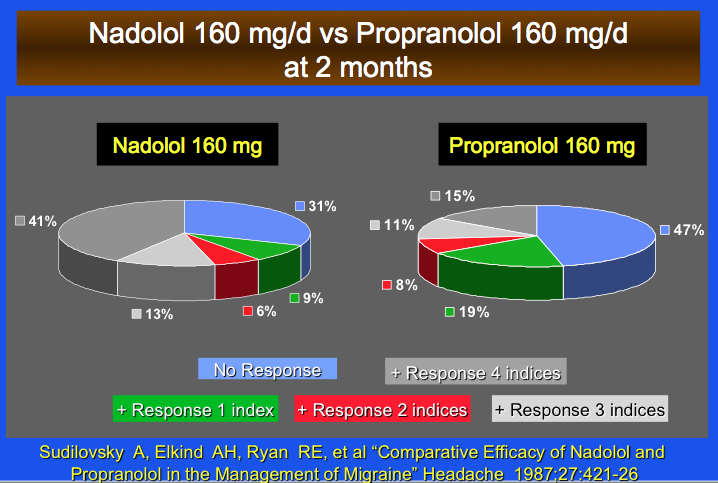
Even if headache scores at the end of the trial were similar, you can see by looking at the pie graph that discloses each component of the headache score that there are important differences.
For instance, the blue segment of the pie graph indicates that the number of non-responders to propranol (47%) was substantially greater than non-responders to nadolol (31%). Perhaps more importantly, the number of subjects who had a favorable response in all 4 components of the headache index (frequency, intensity, number of headache days, need for backup medication) was distinguishably more favorable for nadolol (41%) than propranolol (15%).
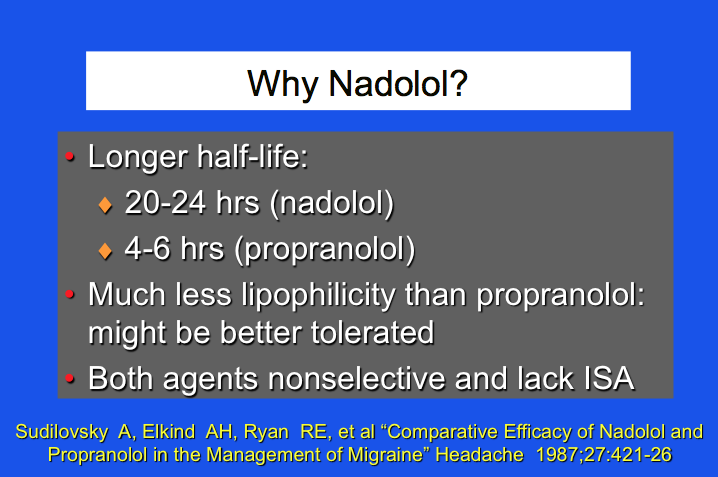
In this particular trial, nadolol was also better tolerated: The discontinuation rate due to adverse events was more than twice as great in subjects treated with propranolol (9.1%) compared to nadolol (4.1%).
What’s the “Take Home?”
The “headache score” or “headache index” is a useful tool because it contains the clinical endpoints most important to physicians and our patients. However, because it is a composite, it can mask some deficits. In a head-to-head trial between propranolol and nadolol, a favorable response in each of the headache score was seen much more frequently in those treated with nadolol, which was also better tolerated. Even though we might be tempted to say “beta-blocker/shmeta-blocker,” it appears that, especially in persons who have not experienced a positive response to propranolol, consideration of another beta-blocker is certainly reasonable.
Reference:
Sudilovsky A, Elkind AH, Ryan RE, et al. Comparative efficacy of nadolol and propranolol in the management of migraine. Headache. 1987;27:421-426.