
Pearls of Wisdom: Identifying Microalbuminuria
Alma is a 62-year-old hypertensive Hispanic female with diabetes who has achieved goal blood pressure, blood glucose, and lipids levels. Her current medications include metformin and glipizide for diabetes mellitus, ramipril and amlodipine for hypertension, and atorvastatin for lipids.
Guidelines from the American Diabetes Association recommend an annual screening for urinary protein excretion. A dipstick urine test in the office is negative. Her estimated glomerular filtration rate (eGFR) is 62 mL/min, which has been stable for 2 years.
Which of the following statements regarding her in-office urine dipstick test is true?
A. No protein is no protein.
B. Standard office urine dipstick testing only detects macroalbuminuria; further testing is needed.
C. Standard office urine dipstick testing detects both microalbuminuria and macroalbuminuria.
D. Because the patient has relatively good kidney function (stage 2 chronic kidney disease), no urinary protein testing is required.
What is the correct answer?
(Answer and discussion on next page)
Louis Kuritzky, MD, has been involved in medical education since the 1970s. Drawing upon years of clinical experience, he has crafted each year for almost 3 decades a collection of items that are often underappreciated by clinicians, yet important for patients. These “Pearls of Wisdom” often highlight studies that may not have gotten traction within the clinical community and/or may have been overlooked since their time of publishing, but warrant a second look.
Now, for the first time, Dr Kuritzky is sharing with the Consultant360 audience. Sign up today to receive new advice each week.
Answer: Standard office urine dipstick testing only detects macroalbuminuria; further testing is needed.
Evolving staging for chronic kidney disease (CKD) take into account both level of protein excretion and estimated glomerular filtration rate (eGFR). Both elements are important since a declining GFR or the presence of abnormal amounts of urinary protein predict not only further decline in renal function, but also total mortality in both type 1 and type 2 diabetes mellitus, cardiovascular endpoints in diabetics and non-diabetics, and the progression of blood pressure in hypertensive patients.1 So, urinary protein is a good marker of existing or impending pathology.
___________________________________________________________________________________________________________________________________________________________________
RELATED CONTENT
Diabetic Kidney Disease in the Elderly: Diagnosis, Treatment Goals
Diagnosis, Treatment Goals, and Management of Diabetic Kidney
___________________________________________________________________________________________________________________________________________________________________
Nephropathy
The terminology of nephropathy is somewhat unwieldy. Normal adults do not excrete more than 30 mg of albumin in 24 hours, although even in healthy individuals fever, acute illness, or vigorous physical activity can induce transient elevations of urinary albumin >30 mg within 24 hours.
Any persistent urinary excretion of protein >30 mg in 24 hours reflects renal pathology, which most commonly defects in the glomerular basement membrane due to hypertension of diabetes—allowing the otherwise extraordinarily efficient protein filtration system to leak.
At the stage labeled microalbuminuria (30 mg/24 hours to 300 mg/24 hrs), the literature has shown that improvement of intraglomerular hemodynamics with angiotensin-converting-enzyme (ACE) inhibitors or angiotensin II receptor blockers (ARBs) can stop, or even reverse the pathologic leakage. Microalbuminuria does not refer to the leakage of small albumin, rather it refers to small amounts of albumin being excreted.
Screening for Microalbuminuria1

Untreated, microalbuminuria often progresses to macroalbuminuria, which is associated with much more rapid decline in renal function and ultimately may progress to the need for dialysis. Macroalbuminuria (also known as frank nephropathy) is diagnosed when urinary albumin excretion is >500 mg/24 hours.
By the time glomerular filtration function has declined to the point of reflecting macroalbuminuria, progressive decline in renal function is certain. Although interventions (eg, blood pressure control, diabetes control, ACE inhibitor treatment, ARB treatment) can slow the decline of renal function even at this stage, they cannot stop the decline. Hence, it is valuable to be able to diagnose abnormal albumin excretion at its earliest stage microabluminuria, during which it is much more amenable to intervention.
In-Office Testing
Traditional office dipstick testing kits detect protein excretion in the urine, but only when it is >500 mg/24 hrs. Thus, they are not useful for the detection of microalbuminuria. Several methods of testing allow identification of urinary protein excretion. Even we are interested in the 24-hour excretion, collection of a 24-hour specimen—unless done in the hospital—has been shown to be sufficiently inconsistent that other now preferred methodologies—such as, a timed urine specimen (eg, 4 hours), or most commonly a “spot urine” from which an albumin-to-creatinine ratio can be calculated.
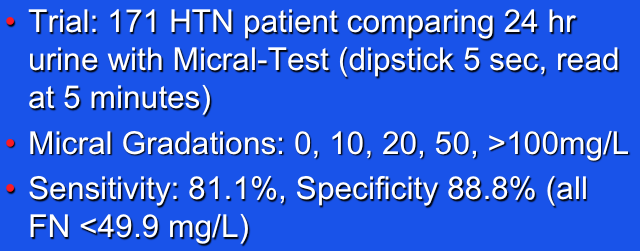
There is another tool that could be applied to provide immediate point-of-care assessment for microalbuminuria: a specialized urinary dipstick, such as Micral. Specialized dipstick testing with such tools has been shown to have greater than 80% sensitivity for the detection of even the most modest levels of microalbumin, and these methods are relatively inexpensive (<$10/test).
Screening Simplified1
A negative test with microalbumin dipstick testing has an extraordinarily high negative predictive value: Your patient has a negative Micral test? The likelihood of missed microalbuminuria is <5%. The value of being able to immediately determine the presence/absence/severity of urinary protein excretion during a regular office visit can be substantial. Unfortunately, third-party reimbursement for specialized microabuminuria dipstick testing has been inconsistent and may not fully cover the costs of the testing.
What’s the “Take Home”?
Urinary protein excretion is a harbinger of decline in renal function and a marker for not only impending renal disease, but also cardiovascular endpoints and total mortality. The recommendations from the American Diabetes Association to obtain annual urinary protein excretion seems sensible and accessible through either point-of-care testing or formal laboratory testing.
Reference:
1. Gerber LM, Johnston K, Alderman MH. Assessment of a new dipstick test in screening for microalbuminuria in patients with HTN. Am J Hypertens. 1998;11:1321-1327.