
Pearls of Wisdom: Hyperkalemia
Lorelei is a 56-year-old recently menopausal woman with a BMI of 25 and a history of type 2 diabetes, hypertension, and dyslipidemia. She comes to your office for an annual check of her electrolytes.
She is currently taking a combination of chlorthalidone and atenolol and reports no symptoms. She has been able to successfully control her blood pressure with this medication for the past 3 years.
Knowing that chlorthalidone is longer acting and more potent than hydrochlorothiazide, you run an annual complete metabolic profile to monitor for possible hypokalemia and check her renal function.
The laboratory tests show that her potassium, which has been stable over the past 3 years, is 5.9 meq/dL (normal <5.5 mmol/dL). The lab slip does not indicate that it was a difficult draw or any evidence of hemolysis.
Which of the patient’s recent medications may account for her hyperkalemia?
A. Over-the-counter loratidine, which the patient began 2 weeks ago for mild allergy symptoms
B. Trimethoprim-sulfamethoxazole, which the patient was prescribed to treat a urinary tract infection 1 week prior
C. Beta blocker eye drops prescribed by her ophthalmologist for glaucoma 2 weeks prior
D. Vaginal estrogen cream that the patient had recently used to treat atrophic vaginitis
What is the correct answer?
(Answer and discussion on next page)
Louis Kuritzky, MD, has been involved in medical education since the 1970s. Drawing upon years of clinical experience, he has crafted each year for almost 3 decades a collection of items that are often underappreciated by clinicians, yet important for patients. These “Pearls of Wisdom” often highlight studies that may not have gotten traction within the clinical community and/or may have been overlooked since their time of publishing, but warrant a second look.
Answer: Trimethoprim-sulfamethoxazole.
Treatment with trimethoprim-sulfamethoxazole (TMP-SMX) in persons with HIV requires high-dose therapy—as much as 20 mg/kg. However, several cases of hyperkalemia associated with TMP-SMX administered in typical doses—as in the treatment of a urinary tract infection—have also been documented.1
The Research
In order to elucidate the relationship between standard dose TMP-SMX and hyperkalemia, researchers compared potassium levels in persons taking TMP-SMX (<320/1600 mg/d) with study subjects who had received other antibiotics.
The Results
The data showed that TMP-SMX was associated with a mean potassium increase of 1.21 meQ/dL as compared to the controls and that 21% of patients achieved a potassium level greater than 5.5 mmol/dL.
Hyperkalemia and TMP-SMX: Results1
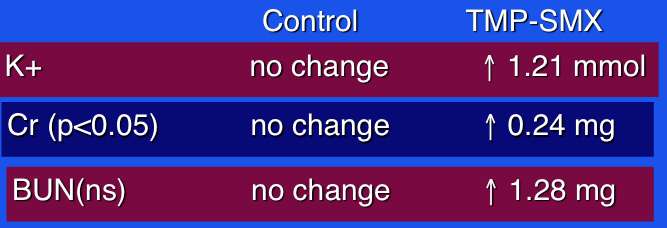
Researchers concluded that hyperkalemia is not widely recognized as a consequence of TMP-SMX, and noted that persons with underlying renal insufficiency are more prone to develop hyperkalemia. If clinicians have concerns about possible hyperkalemia, they can monitor the patient for 2 to 7 days (generally when the peak occurs).
The mechanism of hyperkalemia is unknown. Because trimethoprim is structurally similar to the potassium-sparing diuretic amiloride, that is the attributed pathophysiology.
What’s the “Take Home”?
TMP-SMX is commonly used in a diversity of infectious disease scenarios. Clinicians should be aware that it can cause hyperkalemia. Persons with impaired renal function or baseline levels of potassium that are elevated merit closer monitoring.
Reference:
1. Alappan R, Perazella MA, Buller GK. Hyperkalemia in hospitalized patients treated with trimethoprim-sulfamethoxazole. Ann Intern Med. 1996;14(3):316-320.