
Pearls of Wisdom: Actinic Keratosis
Question: Angus, a 66-year-old farmer, comes in complaining of itchy bumps on his arms and dorsal hands. Over the last 5 years, he has received cryotherapy for individual actinic keratosis on 8 different occasions. Angus asks you, “Look doc, I don’t want you to take this personal or nothin’, but is there somethin’ I could do for these pesky critters instead o’ comin’ in to see you every few months for a freeze job when new ones pop up?”
Cryotherapy is the most commonly procedure for management of actinic keratosis (AK). Which methodology would provide the most expedient field therapy for our patient Angus?
A. Topical 5-fluoruracil (eg, Effudex)
B. Topical imiquimod (eg, Aldara)
C. Topical ingenol mebutate (eg, Picato)
D. Topical diclofenac (eg, Solaraze)
What is the correct answer?
(Answer and discussion on next page)
Louis Kuritzky, MD, has been involved in medical education since the 1970s. Drawing upon years of clinical experience, he has crafted each year for almost 3 decades a collection of items that are often underappreciated by clinicians, yet important for patients. His “Pearls of Wisdom” as we like to call them, have been shared with primary care physicians annually in an educational presentation entitled 5TIWIKLY (“5 Things I Wish I Knew Last Year”…. or the grammatically correct, “5 Things I Wish I’d Known Last Year”).
Now, for the first time, Dr Kuritzky is sharing with the Consultant360 audience. Sign up today to receive new advice each week.
Answer: Topical ingenol mebutate (eg, Picato)
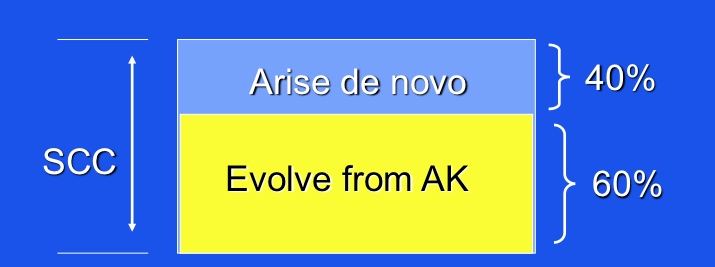
Many clinicians have likely underestimated the significance of actinic keratosis (AK). Whereas they are commonly viewed as a “nuisance” dermatosis, experts suggest that as many as 60% of squamous cell carcinomas (SCC) arise from AK.1 Indeed, some have even said that AK is actually SCC in situ, not just a “benign variant.”
Literature indicates that primary care clinicians are less familiar with AK than SCC and basal cell carcinoma (BCC).1 Because it is not possible to discern which AK will evolve to SCC and because patients often harbor many AK at the same time, there is some wisdom to apply what is called field therapy—ie, instead of simply doing a destructive process, such as cryotherapy, for an individual lesion, why not apply a topical agent to a sun-exposed area noted to contain AK, thereby not only destroying the original AK of interest and also any incipient AK.
______________________________________________________________________________________________________________________________________________________
RELATED CONTENT
Actinic Keratosis
Can You Identify These Sun-Induced Lesions?
______________________________________________________________________________________________________________________________________________________
Prevalence of AK
If you want to blame someone for AK, you may need to look to Coco Chanel, creator of the famous perfume magnate. Prior to her commercial influence, beauty in women was portrayed as dependent upon creamy white skin, not “tainted” by the sun. As a result, lower class, working women, who might have to work outside and develop a suntan, were not runway material. On the other hand, elegant women would protect their skin from the sun with extravagant wide-brimmed hats. However, a commercial campaign stimulated by Coco Chanel’s endorsement of the “beauty of tanned skin” in the 1920s created ripples of effect that even impact us today; tanned skin is now viewed as healthy and athletic.
Disease Path
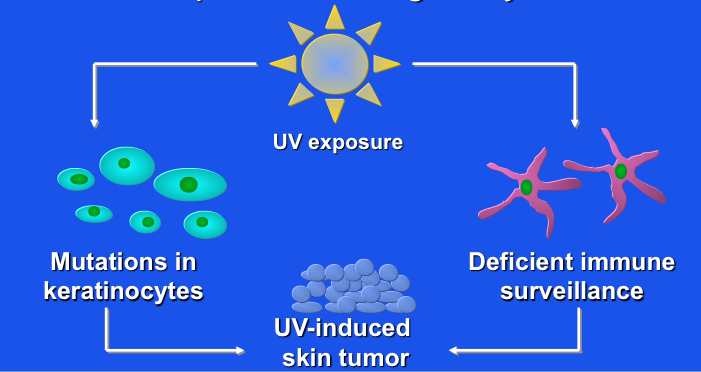
The storyline of AK and SCC development has been fairly well worked out. Both UVA and UVB conspire to induce mutations in sun-exposed keratinocytes.2 Normally, the p53 suppressor gene performs surveillance on cells containing potentially harmful or dysfunctional mutations, shutting off such “broken” cells off by either putting them to sleep (induced senescence) or directing them through the process of apoptosis (programmed cell death), either pathway ultimately resulting in their removal from active cell processes.
Unfortunately, UVA and UVB exposure can also damage the p53 suppressor gene functions, so that it is no longer fully active in discarding abnormal cells. When this happens, mutated cell lines are allowed to proliferate—resulting in AK and SCC.
Typically, when a patient presents with a problematic lesion or 2, those are not the only relevant dermatoses to be considered. Follow-up of patients with AK at baseline—indicative of either their prior excessive exposure to sunlight, their proclivity to develop AK, or both—shows that new lesions develop over time, even when target lesions are removed. Some of the new lesions were in the early process of development when the target lesions were removed, others reflect totally new AK, and some AK may have been refractory to treatment and have recurred. In any case, AK appears to beget more AK.3
Prevalence: What Should We Focus On?5
Geographic Reconsideration
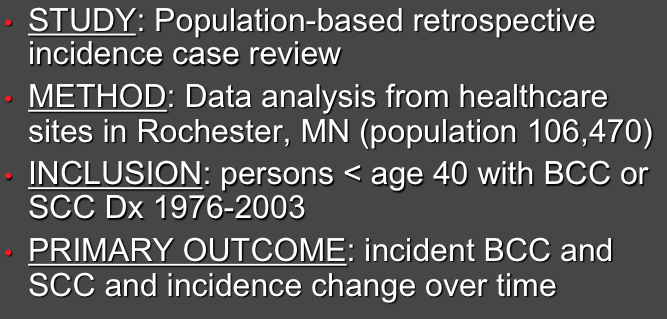
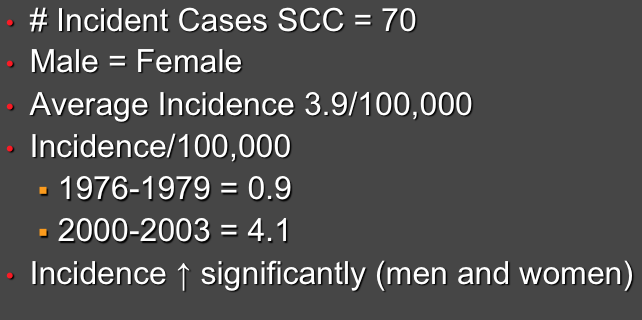
Although we tend to think of AK and SCC as problematic only in the sun-drenched part of our universe (eg, Florida and Arizona), increases in SCC have even been seen in communities where high-volume sun exposure is not an expectation. A study from Olmstead County, MN (home of the Mayo Clinic) found a surprising increase in frequency of SCC even in very young persons (age <40 years). Over a 27-year window of observation, there was a 4-fold increase in SCC incidence within this population!4
SCC in Persons <404
Therefore, regardless of geography, clinicians need to be informed about best management techniques for identification and eradication of AK, SCC, and BCC.
SCC in Persons <40: Results4
Treatment
Our patient, Angus, would like something to reduce the frequency of treatments. Fortunately, we have numerous effective topical agents that can be used not only to destroy the target lesions that were sufficiently bothersome to bring him into the office, but also are effective to address incipient AK and prevent their further development, which in turn reduces the likelihood that he will have to return for further treatments.
Mechanisms of UV-Induced Epidermal Malignancy
Amongst the treatments used commonly in the primary care setting, imiquimod (Aldara), 5-flourouracil (Effudex), and diclofenac (Solaraze) are all acceptable choices. Each has been shown to eradicate the majority of target lesions (as well as lesions not visible at the time of presentation). The limitation of each of these agents is that application regimens typically involve weeks to months of treatment.
______________________________________________________________________________________________________________________________________________________
RELATED CONTENT
Skin Disorders in Older Adults: Benign Growths and Neoplasms
Seborrheic Keratosis
______________________________________________________________________________________________________________________________________________________
Fortunately, a new, very simple to use agent is available that requires on 2-3 days of application, with success rates for AK eradication similar to other agents.
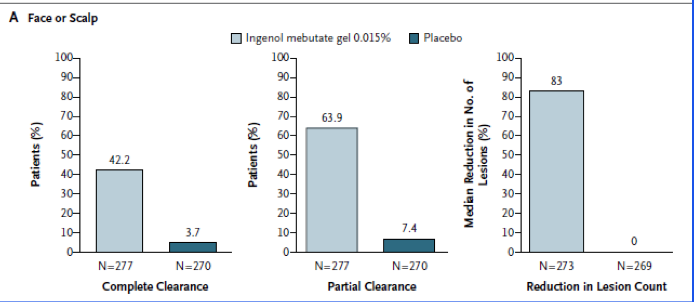
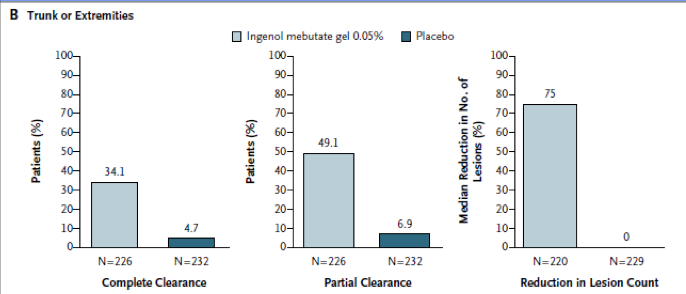
Ingenol mebutate (Picato) is applied to the area of interest for 2 days (face, using lower strength gel 0.015%) or 3 days (trunk and extremities, using higher strength gel 0.05%). Note: Before prescribing ingenol, clinicians should visit the pharmaceutical company’s website because coupons for very significant price reduction are available regardless of need status.
Ingenol Mebutate Gel: A New Field Rx6
What’s the “Take Home”?
AK probably doesn’t get the respect it deserves. If experts are correct that AK is actually SCC in situ, then we should probably be doing a better job of field therapy to eradicate as many AK and incipient AK incidents as possible. Cryotherapy does satisfy a patient’s request to address an individual lesion, but omits the rest of the lesions that may emerge in the near future. A variety of good choices for topical field therapy are available. If expedience is the issue that drives the therapeutic direction, there is no method of field therapy that works with as simple an administration time as 2-3 days (ingenol mebutate).
- Rosen R, Lebwohl MG. Prevalence and awareness of actinic keratosis: barriers and opportunities. J Am Acad Dermatol. 2013;68(Suppl 1):S2-S9.
- Berman B, Cockerell CJ. Pathobiology of AK: UV-dependent keratinocyte proliferation. J Am Acad Dermatol. 2013;68(Suppl 1):S10-S17.
- Budtz PE. Expectations of human epidermal kinetic homeostasis. Br J Dermatol. 2006;114:645–650.
- Christenson LJ, Borrowman TA, Vacon CM, et al. Incidence of BCC and SCC in a population younger than 40 years. JAMA. 2005;294:681-690.
- Stengel RM, Stone SP. Sun-damaged skin: diagnosis and treatment of nonmelanoma skin cancer. Managing Common Skin Diseases. 2003:19-24.
- Lebwohl M, Swanson N, Anderson LL, et al. Ingenol mebutate gel for actinic keratosis. N Engl J Med. 2012;366:1010-1019.