
Interactive Quiz: Confusion and Speech Difficulty
Welcome to Neurology Consultant's latest interactive diagnostic quiz. Over the next few pages, we'll present a case and ask you to make the diagnosis and treat the patient. Along the way, we'll provide details about the case, and at the end, we'll share the patient's outcome.
Ready to get started?
First let’s meet the patient.
A 39-year-old woman with a medical history of morbid obesity, hypertension, and type 2 diabetes mellitus presented to the emergency department (ED) 8 hours after the onset of right upper extremity numbness and weakness, speech difficulty, and confusion.
The patient was afebrile, with a blood pressure of 143/96 mm Hg, a heart rate of 110 beats/min, a respiratory rate of 16 breaths/min, and oxygen saturation of 100% on room air as measured by pulse oximetry.
Physical examination revealed normal heart sounds without murmurs, and tachycardia but regular rhythm. The lungs were clear to auscultation bilaterally, and the abdomen was soft, nontender, and nondistended with normal bowel sounds.
Neurological examination findings were significant for right upper extremity strength, 3/5; right lower extremity strength, 4/5; and left upper and lower extremity strength, 5/5. There were no sensory deficits. The patient had a National Institutes of Health Stroke Scale (NIHSS) score of 3 (corresponding with minor stroke) based on the presence of minor facial palsy, right arm drift, and mild to moderate dysarthria.
Are you correct? >>
Answer: Admit the patient to the hospital
Laboratory test results were significant for hyperglycemia and leukocytosis without infectious symptoms. Findings of computed tomography (CT) and CT angiography (CTA) of the head were negative for any abnormalities. The patient was given aspirin and was admitted to the hospital for a neurology consult and magnetic resonance imaging (MRI), given her persistent neurological changes.
Findings of an MRI scan of the head were significant for multifocal bilateral subacute infarcts, predominantly scattered throughout the left cerebral hemisphere with superimposed multifocal remote infarcts, and vessel occlusion (Figures 1-3).
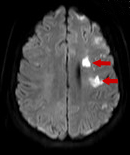
Figure 1
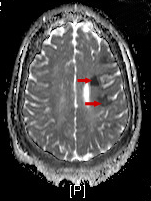
Figure 2

Figure 3
Cerebral angiography was then performed to further clarify the MRI findings; the results showed severe stenosis of the right and left middle cerebral and anterior cerebral arteries (Figure 4).
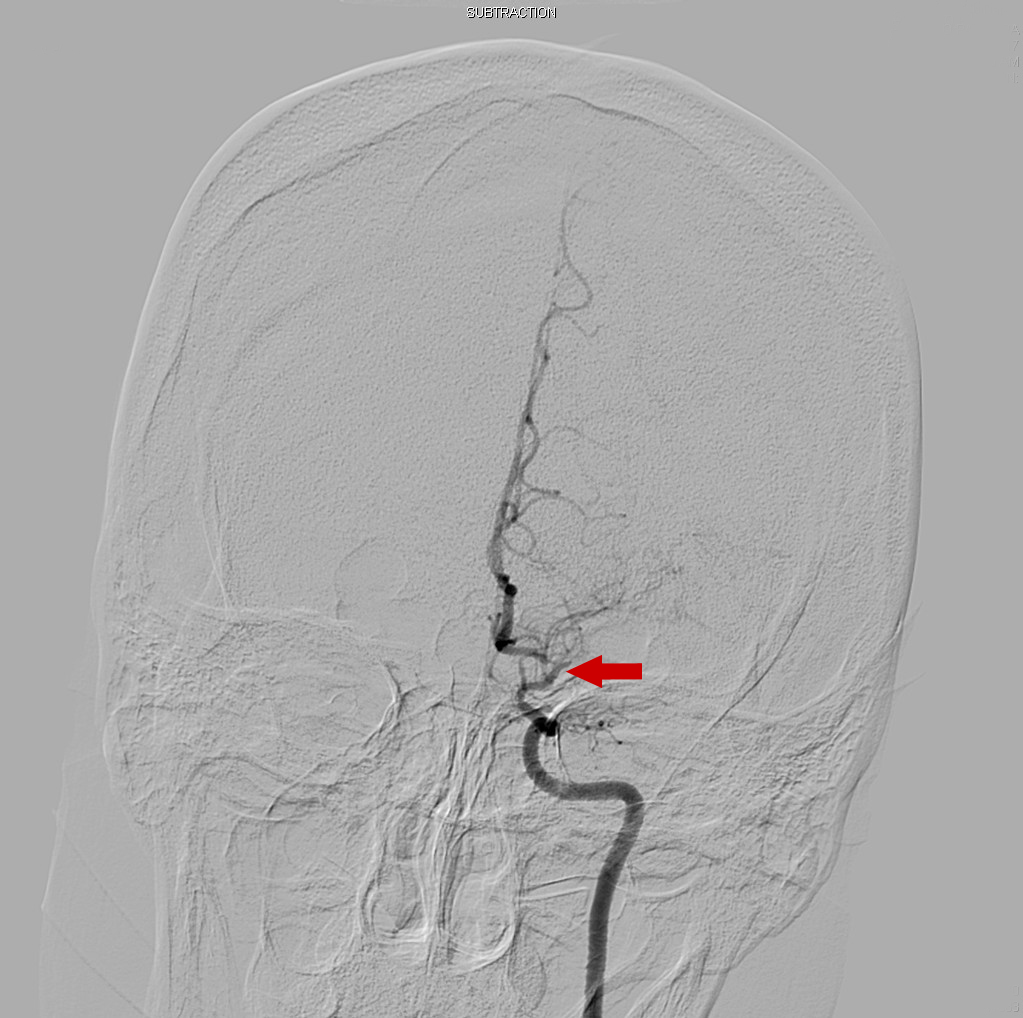
Figure 4
Are you correct? >>
Answer: Moyamoya disease
A consulting neurosurgeon determined that the patient’s disease pattern was consistent with moyamoya disease. While no acute inpatient intervention was performed, the neurosurgeon recommended aspirin, a statin, and encephaloduroarteriosynangiosis (EDAS).
During this hospitalization, the patient also received a diagnosis of Graves disease based on a finding of elevated thyroid antibodies and was started on appropriate treatment before being discharged.
In the following months, the patient underwent left- and right-sided EDAS and had a complicated postoperative course, with opioid overdose and seizure activity for which she was placed on levetiracetam therapy.
Approximately 7 months later, the patient again presented to the ED with worsening right-sided facial droop, dysphagia, and dysarthria with an onset several hours prior to arrival.
On physical examination, she had right facial droop, tongue deviation, and slurred speech with an NIHSS score of 4. Neurological and physical examination findings were otherwise normal. Given the patient’s extensive neurological history, we obtained a medical workup and imaging to determine whether this was a postoperative complication, hemorrhage, or new infarction secondary to severe disease state.
A CT scan of the head revealed a slight increase in volume loss in the left hemisphere compared with the right, and chronic ischemic changes again were identified bilaterally. Results of further workup in the ED were significant for hyperglycemia secondary to poorly controlled diabetes and tobacco use prior to the onset of symptoms.
Are you correct? >>
Answer: Yes, the patient should be admitted to the hospital.
The patient was admitted to the hospital for MRI and a neurology/neurosurgery consult.
The patient’s hospital course during this admission was uncomplicated, and MRI findings were significant for small areas of diffusion signal abnormality in the right frontal lobe, which were thought to represent areas of subacute infarct; otherwise, there was no significant change from scans taken during her previous hospitalization.
The patient was restarted on aspirin and statin therapy and received fluid boluses, since it was felt that her symptoms were a result of hypotension/hypoprofusion or, secondarily, tobacco-induced vasospasm. Her symptoms had mildly improved on discharge, and she was counseled on the dangers of tobacco use and dehydration, given her rare and serious clinical diagnosis of moyamoya disease.
Are you correct? >>
Answer: 0.086 per 100,000 population
Moyamoya disease is a cerebrovascular disorder characterized by bilateral progressive stenosis and occlusion of the terminal portions of the internal carotid artery and accompanying typical netlike collateral vessels in the basal ganglia.
The incidence of moyamoya disease is relatively higher among people of Asian heritage, with the highest occurrence rate in Japan, where the reported prevalence is 0.35 per 100,000 population.1 However, in the Western United States, the prevalence is 0.086 per 100,000 population.1 Nevertheless, the prevalence of the disease in the United States may be increasing.2 The condition has a female predominance and a bimodal age distribution involving the first and fourth decades of life.1
Authors and References >>
Authors:
Anne Lally, DO, and David Effron, MD
MetroHealth Medical Center, Cleveland, Ohio
Citation:
Lally A, Effron D. Moyamoya disease [published online October 29, 2018]. Neurology Consultant. https://www.consultant360.com/article/neurology/neurology/moyamoya-disease.
References:
- Ismail I, Al-Khafaji K, Mutyala M, et al. ‘Smoke in the air’: a rare cerebrovascular cause of neurological signs and symptoms in a young adult. J Community Hosp Intern Med Perspect.2015;5(3):27664.
- Starke RM, Crowley RW, Maltenfort M, et al. Moyamoya disorder in the United States. Neurosurgery. 2012;71(1):93-99.