

Uncontrolled Asthma: A Woman With Worsening Dyspnea and Recurrent Exacerbations
Kartik V. Shenoy, MD |Temple Lung Center, Temple University, Philadelphia, Pennsylvania
A 56-year-old woman with asthma diagnosed 2 years ago presented to your office with daily cough, wheezing, and dyspnea on exertion. In the last year, she has had 3 exacerbations requiring visits to urgent care for oral corticosteroids. Her exacerbations had caused her to miss several days of work each time. She stated that she needs her rescue inhaler 3 times per week, and she has woken up a few nights per month with asthma symptoms.
Her asthma symptoms are maintained with fluticasone, 500 mg salmeterol, 50 mg dry powder inhaler 1 puff twice a day and montelukast 10 mg once daily to prevent asthma exacerbations. She has a medical history of gastroesophageal reflux disease and hypertension, both of which are well controlled. She is taking 20 mg of omeperazole in the morning before eating her breakfast and 10mg of amlodipine once daily. She was referred to you for further management.
You conducted pulmonary function testing, results of which are detailed in the Figure, and you found her results are consistent with airflow obstruction with significant bronchodilator response.
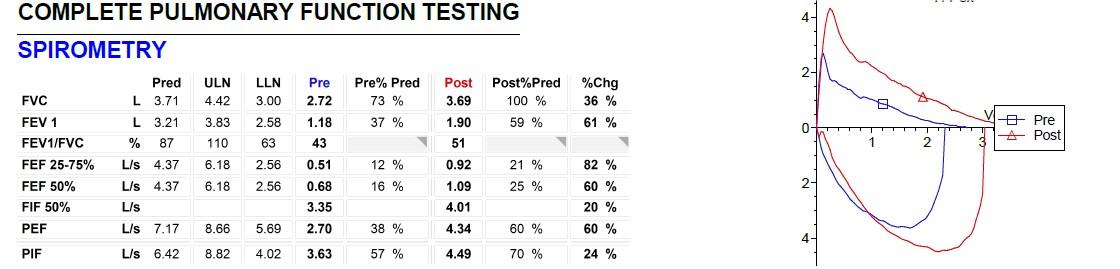
Figure. Pulmonary function data were consistent with airflow obstruction with significant bronchodilator response (ie, improvement of FEV1 by > 12% and > 200 ml).
You also reviewed her inhaler technique, as poor technique may lead to exacerbation, and you found it is excellent. You prescribed tiotropium as an add-on therapy to relax the smooth muscles around the airways and assured the patient that her comorbidities remain well controlled.
You followed her clinical course over the next 12 weeks. She has returned to your office after another visit to urgent care where she was prescribed oral corticosteroids for 5 days. Her symptoms of cough and wheezing improved with the oral corticosteroids, but she still needs to use her rescue inhaler 2 to 3 times per week, and still feels limited by her asthma symptoms.
You agree with her previous diagnosis of asthma and consider her to have severe asthma given that she is still experiencing exacerbations while on a high-dose inhaled corticosteroid plus an additional controller medication, her comorbidities are controlled, and her adherence and inhaler technique are good.