
A Young Girl Complains of Left Ankle Pain
A 12-year-old female comes to your office complaining of left ankle pain. Her mother states that she was at the playground when she jumped down from the high bars and has been in pain ever since. The patient is otherwise healthy.
History
The past medical history is noncontributory. The patient does not have history of other fractures.

Figure 1. A frontal radiograph of the left ankle demonstrates a linear lucency through the middle third of the epiphysis consistent with a fracture. This fracture extends proximally and laterally to the physeal plate.
Figure 2. An oblique radiograph of the left ankle demonstrates a linear lucency through the middle third of the epiphysis consistent with a fracture. This fracture extends proximally and laterally to the physeal plate.
Physical Examination
The patient has mild tachycardia; her respiratory rate, blood pressure, and temperature are all within normal limits.
Examination of the left ankle demonstrates moderate soft tissue swelling with focal tenderness in the region of the distal tibia. Since a fracture is suspected, 3 views of the left ankle are ordered.
Laboratory Tests
Frontal, lateral, and oblique radiographs of the left ankle reveal a linear lucency through the epiphysis of the distal tibia (Figures 1-3). This extends to the physeal plate, where there is mild widening.
The CT images clearly confirm the abovementioned findings (Figures 4 and 5).

How would you diagnose this patient?
A. Infection/osteomyelitis
B. Traumatic fracture
C. Stress fracture
D. Pathologic fracture
E. Insufficiency fracture
(Answer and discussion on next page)
 Answer: Traumatic Fracture
Answer: Traumatic Fracture
In this case, a traumatic fracture occurred, where the excessive forces were exerted on healthy bone. This is consistent with a Salter-Harris type III fracture. The CT images clearly demonstrate the fracture and communication with the physeal plate shows that the fracture is minimally displaced.
Pediatric Fractures
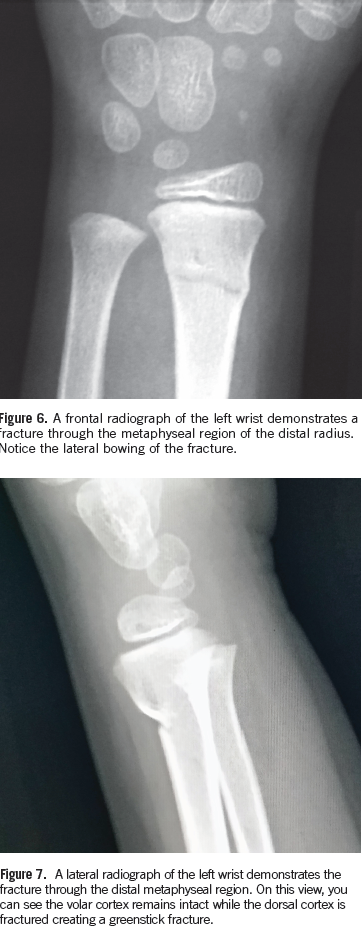
Fractures in the pediatric population are different in many ways than in adults. The pediatric population has a stronger more vascular periosteum (ie, lining of the bone). This typically leads to nondisplaced fractures that heal very rapidly due to the strength of the periosteum. Additionally, the bones in the pediatric population are softer and more pliable than those in the adult population. Frequently, there can be incomplete fractures observed in the pediatric population, such as when the cortex on 1 portion of the bone is fractured and other portions remain intact known as the greenstick fracture (owing its name to the similarity that occurs with a healthy tree branch). If one tries to break the branch, it only breaks on 1 side due to its pliable composition (Figures 6 and 7).
Classification
The other issue with fractures in the pediatric population is the presence of the physeal plate. The physeal plate is a point of weakness in the osseous structures and is often associated with fractures.
In fact, this is so common that there is a classification system related to the fractures of the physeal plate (Figure 8).
• Salter-Harris type I refers to fractures through the physeal plate.
• Salter-Harris type II refers to fractures through the physeal plate and the metaphysis of the bone.
• Salter-Harris type III refers to fractures involving the physeal plate, and epiphysis.
• Salter-Harris type IV refers to fractures involving the metaphysis, physeal plate, and the epiphysis.
• Salter-Harris type V refers to compression fractures of the physeal plate.
Differential Diagnosis
The history of abrupt injury as well as the absence of fever and cellulitis make infection very unlikely in this case.
A stress fracture occurs when an individual engages in overuse of an extremity or other part of the body, particularly after a period of minimal use, and has chronic repetitive microtrauma that leads to weakening and subsequent fracture of the bone. The classic example for a stress fracture would be a new military recruit who is asked to march 10 miles a day the first week of his training. At the end of the week, he has foot pain and a nondisplaced stress fracture. The patient in this case was not engaging in repetitive activity. In this demographic, dancers and athletic children may be susceptible to this type of injury.
A pathological fracture is a fracture through bone that is abnormal due to an underlying focal lesion. The most common example of this occurs in older individuals with metastatic disease to their bones who develop a fracture—often in the hip/femoral neck, a weight-bearing region of the body. Pathologic fractures can also occur through benign lesions. In children, fractures occur through unicameral bone cysts, enchondromas, and regions of fibrous dysplasia. These pathologic fractures can occur in non-weight bearing regions of the body. The hallmark of a pathologic fracture is a small force resulting in an unexpected fracturing of a bone.
An insufficiency fracture results from a baseline level of insufficient or weakened bone. The underlying bone does not have the typical strength of healthy bone and therefore, fractures with less force. This is most commonly seen in elderly patients and again occurs in weight-bearing regions of the body—classically in the sacrum and in the region of the femoral neck. These can be difficult to diagnose as the fractures are often not displaced. The underlying abnormal bone is usually related to osteopenia or osteoporosis. Rickets can contribute to an insufficiency fracture as can other conditions.

Outcome of the Case
This patient was casted and the fracture healed in 8 weeks without adverse events.
William Yaakob, MD, is a board certified radiologist working in Tallahassee, FL.