
Peer Reviewed
Wide-Complex Tachycardia Associated With Streptococcal Pharyngitis
Authors:
Alan Lucerna, DO; James Espinosa, MD; and Ramy Saleh, DO
Kennedy University Hospital/Rowan University School of Osteopathic Medicine, Stratford, New Jersey
Citation:
Lucerna A, Espinosa J, Saleh R. Wide-complex tachycardia associated with streptococcal pharyngitis. Consultant. 2017;57(8):507-509.
A 39-year-old man presented to the emergency department (ED) for evaluation of sore throat and palpitations. He reported a temperature of 39.8°C at home but was afebrile on presentation. His radial pulse rate was 234 beats/min.
A 12-lead electrocardiogram (ECG) was obtained immediately, the results of which showed wide-complex tachycardia (Figure 1). Given the morphology noted on the ECG, ventricular tachycardia was a concern. The patient was immediately placed on the monitor, and defibrillation pads were placed on his chest. His blood pressure was 133/107 mm Hg, and his respiratory rate was 20 breaths/min. Pulse oximetry revealed an oxygen saturation of 99% on room air.
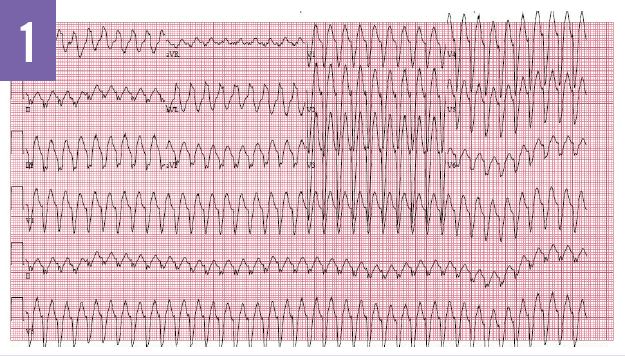
Figure 1. A 12-lead ECG at presentation showing wide-complex tachycardia.
History. The patient denied any relevant medical history. He had no family history of sudden cardiac death, heart disease, arrhythmias, or especially Brugada syndrome. The patient had no congenital heart defects or conduction abnormalities. He did not take any drugs, prescribed or otherwise. He reported no recent travel and no recent illness. He noted that his throat had been painful 1 day prior. He denied chest pain or dyspnea.
Physical examination. The patient appeared to be in no distress. His pharynx was injected, and his tonsils were enlarged but showed no exudates. His lungs were clear to auscultation.
Diagnostic tests. Laboratory test results were notable for a white blood cell count of 17,800/µL, a negative cardiac troponin result, a normal brain natriuretic peptide level, and a positive rapid antigen test result for group A streptococcal (GAS) infection. A chest radiograph showed no infiltrates.
Treatment. The patient was given 325 mg of oral aspirin and was started on intravenous ampicillin-sulbactam. Amiodarone, 150 mg, was administered as an intravenous bolus, followed by an infusion of 1 mg/min. The on-call cardiologist was notified, and a bedside consultation was obtained. Despite being on the amiodarone drip, the patient’s wide-complex tachycardia persisted. Preparations for electrical cardioversion were being initiated when the patient’s rhythm converted to narrow-complex tachycardia consistent with a sinus origin (Figure 2).

Figure 2. A 12-lead ECG after initiation of an amiodarone drip showing sinus tachycardia at 125 beats/min, normal axis, with nonspecific ST-T segment abnormalities.
The patient was admitted to the intensive care unit for continued close monitoring. There was no recurrence of abnormal rhythm during the course of his hospitalization. An echocardiogram showed preserved left-ventricular systolic function with an ejection fraction of 60% to 65%. He was discharged home on amoxicillin-clavulanate, and a statin was prescribed for newly diagnosed hyperlipidemia. A β-blocker was also prescribed.
Follow-up. The patient subsequently underwent cardiac magnetic resonance imaging with and without contrast, the results of which showed a dilated left ventricle without evidence of myocardial infarction (MI) or myocarditis. There were several areas of pericardial thickening. The patient also underwent an exercise stress test, the results of which revealed no evidence of ischemia or arrhythmia.
Outcome of the case. Two months from his initial ED presentation, the patient had a comprehensive invasive electrophysiologic study at another institution. He was able to be induced to have an atrioventricular nodal reentry tachycardia (AVNRT), with 1:1 ventricular conduction, with a left bundle branch block (LBBB) morphology resembling the wide-complex tachycardia seen during his previous ED visit. Radiofrequency ablation was utilized in the areas of the atria mapped to be the source of the inducible AVNRT rhythm. Successful atrioventricular node pathway modification was achieved, which rendered the supraventricular tachycardia noninducible.
Discussion. Streptococcal pharyngitis is the most common bacterial pharyngitis encountered in the ED, accounting for approximately 12 million annual US ambulatory care visits.1 The condition is caused by infection with the GAS bacteria Streptococcus pyogenes. Left untreated, strep pharyngitis can lead to various local and systemic complications, some of which can be life-threatening. One complication, rheumatic heart disease, is estimated to cause approximately 6 million years of life to be lost annually worldwide.1 Between 5 million and 30 million children and young adults worldwide are estimated to have chronic rheumatic heart disease.2
There have been a few reports of cardiac arrhythmias occurring in association with GAS infection. Keller et al3 reported a case of invasive puerperal sepsis due to GAS infection that presented initially with persistent postpartum palpitations and unexplained sinus tachycardia without fever, uterine tenderness, or vaginal discharge. A case of an 89-year-old woman with peritonsillar abscess was reported with associated complete heart block that degenerated to nonsustained ventricular tachycardia.4 Evaluation of this patient did not reveal cardiac ischemia or electrolyte abnormalities to explain her abnormal cardiac rhythm. The author postulated that the complete heart block might have been due to the local compressive effect of the peritonsillar abscess on the vagus nerve, which is housed in the parapharyngeal space.4
In a broader literature search, we encountered a case report of purulent pericarditis that presented with diffuse ST segment elevation on ECG and was shown on pericardial fluid cultures to be caused by a group G streptococcus.5 Shortly thereafter, colonoscopy findings revealed colon cancer. Invasive streptococcal infections reportedly have been shown to cause ST-T segment abnormalities; a few authors have reported cases of group A or group B streptococcal myocarditis resulting in ST segment elevations mimicking an acute MI in young patients.6,7
While our patient received a diagnosis of strep pharyngitis, he did not have a peritonsillar abscess. He had no electrolyte abnormalities or evidence of ischemia. At presentation, a ventricular tachycardia diagnosis was considered and was the target of initial stabilization efforts, given the widened QRS complex on initial ECG. The subsequent electrophysiologic study confirmed an AVNRT with an LBBB to be the underlying rhythm.
AVNRT is common in patients in their 20s and 30s. It is the most common cause of palpitations in patients whose heart has no structural abnormality.8 It can occur paroxysmally but also can be provoked.
Known triggers include alcohol, coffee, or tea ingestion. Our patient denied alcohol use or drug abuse. Given that caffeine is a known trigger, we speculate that substances or conditions that produce a sympathomimetic or catecholinergic response may trigger a reentrant condition, resulting in AVNRT. It can be argued that the temporal association between our patient’s onset of acute pharyngitis and his palpitations demonstrates a clear link between the 2 conditions.
There is a paucity of data in the literature describing GAS pharyngitis and cardiac rhythm disturbances. We believe that our case report illustrates a novel case of strep throat associated with wide-complex tachycardia and AVNRT.
REFERENCES:
- Carrillo-Marquez MA. Bacterial pharyngitis. Medscape. http://emedicine.medscape.com/article/225243-overview. Updated March 17, 2016. Accessed July 12, 2017.
- Chin TK. Pediatric rheumatic heart disease. Medscape. http://emedicine.medscape.com/article/891897-overview. Updated January 3, 2017. Accessed July 12, 2017.
- Keller NA, Guan X, Wiczulis A, Burcher P. Unexplained persistent postpartum palpitations and tachycardia due to group A streptococcus. BMC Res Notes. 2015;8:731.
- Hussain MA. A unique case of quincy complicated by complete heart block and ventricular tachycardia: a case report. Webmedcentral. 2012;3(2):WMC003001.
- Kim NH, Park JP, Jeon SH, et al. Purulent pericarditis caused by group G streptococcus as an initial presentation of colon cancer. J Korean Med Sci. 2002;17(4):571-573.
- Nalmas S, Nagarakanti R, Slim J, Abter E, Bishburg E. Electrocardiographic changes in infectious diseases. Hosp Physician. 2007;43(9):15-27.
- Aguirre JL, Jurado M, Porres-Aguilar M, et al. Acute nonrheumatic streptococcal myocarditis resembling ST-elevation acute myocardial infarction in a young patient. Proc (Bayl Univ Med Cent). 2015;28(2):188-190.
- Cadogan M. AVNRT for two. Life in the Fast Lane. https://lifeinthefastlane.com/avnrt-ecg/. September 30, 2009. Accessed July 12, 2017.