
Peer Reviewed
What’s Behind This 11-Year-Old Girl’s Yearlong History of Knee Pain?
AUTHOR:
Leslie Hoover, CNP
CITATION:
Hoover L. What’s behind this 11-year-old girl’s yearlong history of knee pain? Consultant for Pediatricians. 2015;14(3):127-129.
An 11-year-old obese girl presented to the orthopedic clinic with a history of bilateral knee pain. The girl had visited an urgent care clinic 8 months prior for left knee pain. At that time, she reported 3 days of knee pain, followed by a slip on the ice with no contact with the ground, and then 3 additional days of knee pain. She was limping and had tenderness over the medial knee, including the patella, and reported pain with knee flexion. Anteroposterior (AP) and lateral left knee radiographs at the time were notable for mild soft-tissue swelling with a joint effusion.
She returned to the urgent care clinic 5 weeks later for left knee pain. She had remained on crutches since her initial evaluation at the urgent care clinic. Physical examination revealed diffuse pain with inconsistent location and nature. Range of motion in her left lower extremity was not limited, and no outward signs of trauma were present. She had an exaggerated antalgic gait and kept her leg stiff while ambulating. She was able to flex her knee easily without assistance. Nonsteroidal anti-inflammatory drugs, an ACE wrap, and full weight-bearing were recommended.
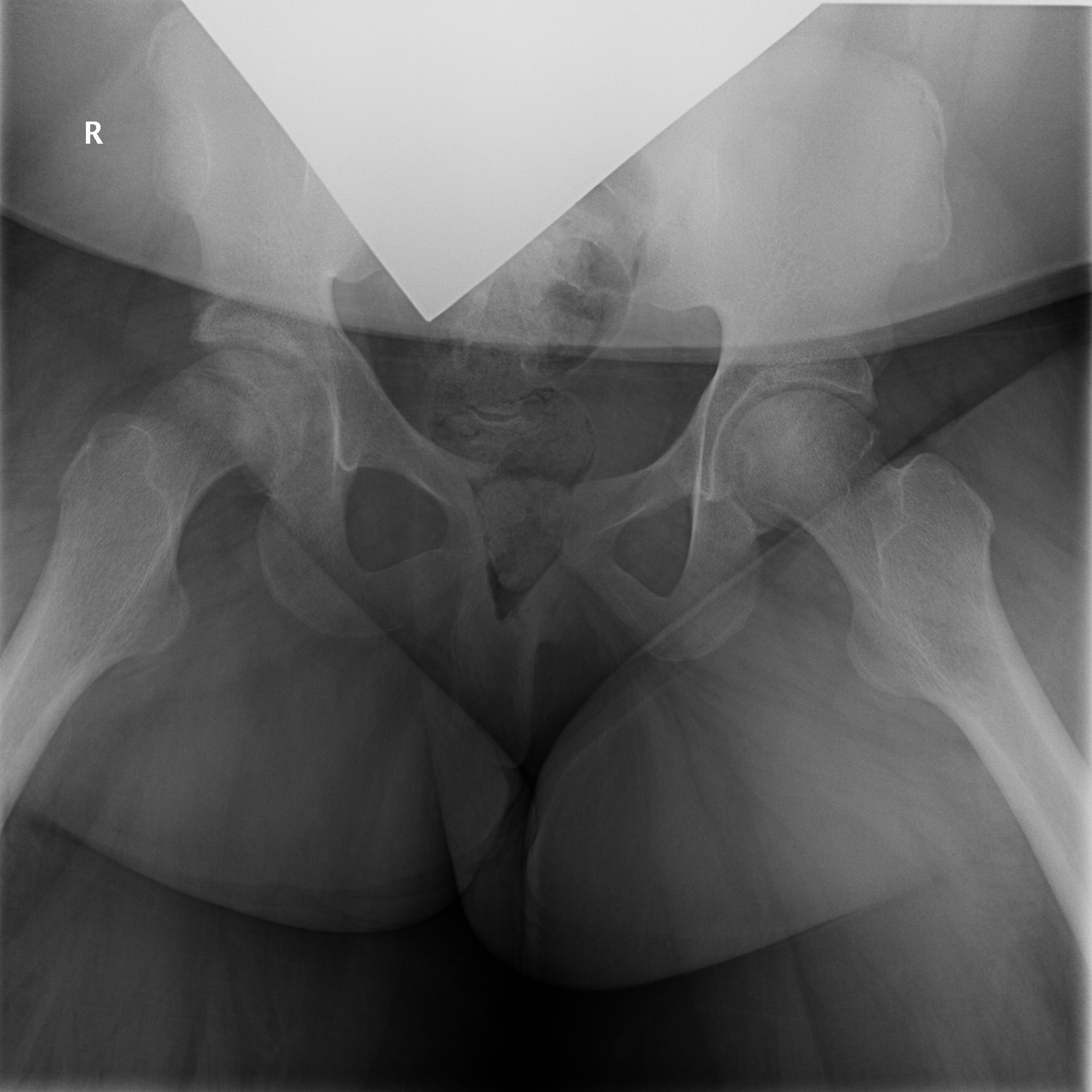
Upon presentation to the orthopedic clinic several months later, her chief concern was chronic right knee pain of 1 year’s duration. She was able to bear weight with crutches. Knee examination findings were unremarkable, but she experienced exquisite pain with log roll on the right lower extremity. AP and frog-leg lateral pelvis radiographs were taken, the latter of which is shown in Figure 1.

Figure 1. Radiographic scan of the pelvis.
(Answer and discussion on next page)
Answer: D, slipped capital femoral epiphysis
AP and frog-leg lateral radiographs of the girl’s pelvis (Figure 1) revealed bilateral slipped capital femoral epiphysis (SCFE). Left-side findings suggested remote, healed SCFE, and right-side findings suggested acute versus subacute SCFE with an open physis. Her past medical history revealed obesity and hyperinsulinemia with evidence of insulin resistance.
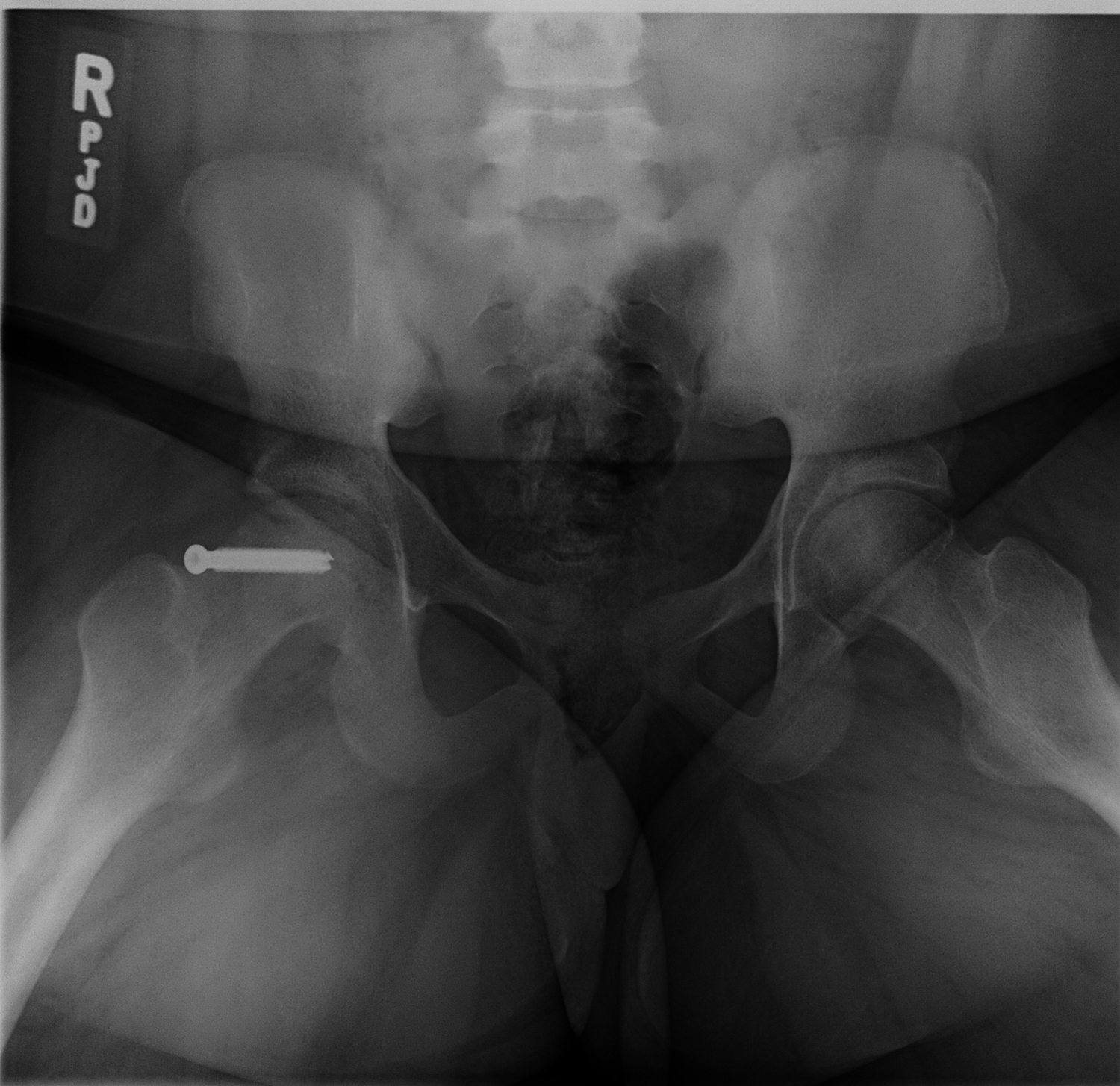
She was admitted directly to the hospital on strict bed rest and later underwent in situ screw fixation of her right SCFE (Figure 2). She was instructed to remain non-weight-bearing on her right leg using crutches for 6 weeks.
At her 2-week postoperative visit, she had been adherent with the restrictions, had been taking hydrocodone-acetaminophen once daily at bedtime, and had been taking ibuprofen intermittently.
Discussion
SCFE typically occurs during adolescence, which is the period of maximal skeletal growth.1 The prevalence of SCFE in the United States is estimated to be from 1 to 11 cases per 100,000 children.2 Its presentation is bilateral in 20% to 40% of cases; in unilateral cases, the second slip usually occurs within the first year.3
Abnormal loading of the hip in children who are obese can lead to anatomic alterations and an increased prevalence of SCFE.4 A correlation between the increasing rates of childhood obesity and the increasing incidence of SCFE in the United States recently has been reported.4,5
SCFE has a greater prevalence in the black, Hispanic, Polynesian, and Native American populations than in the white population.2 It is known to affect males more often than females by a ratio of 1.65 to 1.2
The presenting complaint in cases of stable, chronic SCFE is pain in the groin, which may be referred to the anteromedial aspect of the thigh and knee or may be localized exclusively to the thigh and knee.1,6
Definitive treatment is stabilizing the capital femoral epiphysis to the femoral neck to prevent further slipping. The treatment of choice for cases of stable SCFE is screw fixation.1 Other treatment options include bone graft epiphysiodesis, primary osteotomy through the femoral neck with or without fixation of the epiphysis to the femoral neck, and application of a spica cast.1
Chondrolysis and avascular necrosis are among the complications that may occur spontaneously or that may be related to treatment of SCFE.1
In the primary care, urgent care, or emergency department setting, SCFE must be considered in the differential diagnosis when a child or adolescent complains of knee pain. Evaluation must include a careful examination of the hip, including AP pelvis and bilateral frog pelvis radiographs, to prevent a stable, acute SCFE from developing into a chronic SCFE, which in turn could lead to chronic pain, significant morbidity, and early osteoarthritis.
Leslie Hoover, CNP, is a nurse practitioner in the Orthopedic Department at Nationwide Children’s Hospital, in Columbus, Ohio.
REFERENCES:
- Herring JA. Slipped capital femoral epiphysis. In: Herring JA, ed. Tachdjian’s Pediatric Orthopaedics: From the Texas Scottish Rite Hospital for Children. Vol 1. 5th ed. Philadelphia, PA: Elsevier Saunders; 2014:630-655.
- Lehmann CL, Arons RR, Loder RT, Vitale MG. The epidemiology of slipped capital femoral ephiphysis: an update. J Pediatr Orthop. 2006;26(3):286-290.
- Loder RT, Aronson DD, Greenfield ML.The epidemiology of bilateral slipped capital femoral epiphysis: a study of children in Michigan. J Bone Joint Surg Am. 1993;75(8):1141-1147.
- Murray AW, Wilson NI. Changing incidence of slipped capital femoral epiphysis: a relationship with obesity? J Bone Joint Surg Br. 2008;90(1):92-94.
- Novais EN, Millis MB. Slipped capital femoral epiphysis: prevalence, pathogenesis, and natural history. Clin Orthop Relat Res. 2012;470(12):3432-3438.
- Wabitsch M, Horn M, Esch U, et al. Silent slipped capital femoral epiphysis in overweight and obese children and adolescents. Eur J Pediatr. 2012;171(10):1461-1465.