
What Does Rheumatology Look Like?
Severe Neck Pain Due to Crowned Dens Syndrome
Luciana Funtowicz, MD, Elizabeth B. Windgassen, MD,
and Lester E. Mertz, MD
Mayo Clinic, Scottsdale, AZ
An 81-year-old man presented to the emergency department with a 6-day history of severe neck pain and restricted head movement. He had presented 2 months earlier with similar complaints and was discharged with analgesics. He also reported migratory arthralgias, primarily in the left shoulder, right wrist, and right knee.
His past medical history included diabetes, hyperlipidemia, hypertension, coronary artery disease, renal insufficiency, and myelodysplastic syndrome. His medications were a beta-blocker, statin, aspirin, insulin, and darbepoetin alfa.
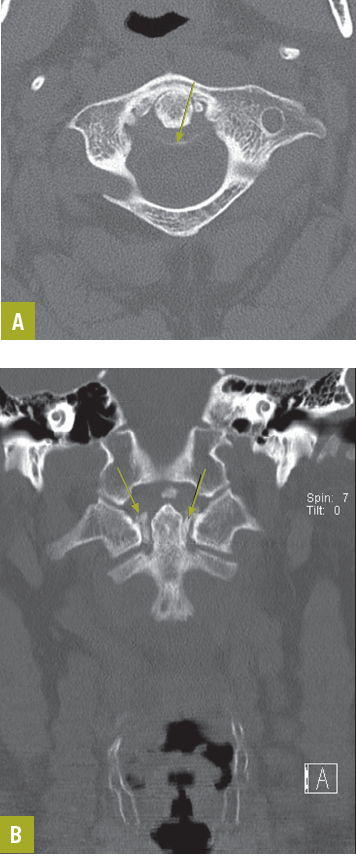
Figure 1. Axial (a) and reformatted (b) CT images demonstrate calcification of the transverse ligament (arrows).
Results of the physical examination were notable for limited range of motion at the neck, left shoulder, right wrist, and right knee because of pain. He had pain on palpation of the right wrist and knee with swelling in both hands and wrists and moderate effusion and warmth of the right knee. He was neurologically intact, and vital signs were stable. His erythrocyte sedimentation rate was elevated at 134 mm/h with a C-reactive protein (CRP) level of 253 mg/L. Other analyses were consistent with his history of diabetes, renal disease, and myelodysplastic syndrome.
He was admitted for pain control and further evaluation. A noncontrast CT scan of the spine revealed moderate degenerative changes. An MRI scan of the spine suggested soft tissue edema along the anterior margin of the upper cervical spine. He was treated with intravenous antibiotics because of concern about possible soft tissue infection, but CT-guided biopsy of the prevertebral space was unrevealing. Results of a lumbar puncture were normal.
A rheumatology consultation was obtained. The consultants’ review of the initial CT scan of the spine noted transverse ligament calcification (Figure 1). A knee joint aspirate revealed calcium pyrophosphate crystals diagnostic of acute pseudogout (Figure 2).
Discussion. The patient’s clinical and radiographic findings, as well as knee joint aspirate, were consistent with the diagnosis of pseudogout, or calcium pyrophosphate crystal deposition disease (CPPD), of the cervicooccipital junction—also known as the crowned dens syndrome. The term derives from the crown-like density surrounding the odontoid process and was first coined in 1985.1 Fenoy and colleagues2 found that up to two-thirds of patients with CPPD exhibit radiographic evidence of involvement of the cervical spine, but symptomatic involvement is relatively rare. Their analysis suggests a mean age at presentation of 70, with women being more likely than men to be affected.2 The presentation is usually acute. Typical symptoms and laboratory findings are severe neck pain with restriction of cervical rotation and a grossly elevated CRP level3; occasionally, fever is present. Crowned dens syndrome has been confused with giant cell arteritis, polymyalgia rheumatica, and meningitis, among other conditions.4
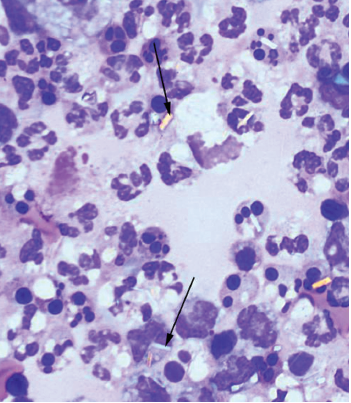
Figure 2. Examination of joint aspitate under polarized light reveals birefringent rhomboid-shaped crystals (arrows).
In this patient, the presence of peripheral joint inflammation ultimately led to the correct diagnosis and initiation of appropriate therapy. The inflammatory edema seen on MRI is typical, with calcifications visible only on CT.
Treatment. Patients with crowned dens syndrome may have spontaneous resolution of symptoms, but typical treatment for CPPD, including NSAIDs, colchicine, or a short course of corticosteroids, may result in more rapid improvement.1,4 Crowned dens syndrome does not require long-term corticosteroid therapy with gradual tapering, as does giant cell arteritis.
Outcome of the case. This patient was treated with a brief course of prednisone but was not given colchicine because of his renal insufficiency. Following initiation of prednisone, a rapid improvement in pain levels and inflammatory markers allowed for his discharge from the hospital. ■
References:
1. Bouvet J, Le Parc J, Michalski B, et al. Acute neck pain due to calcifications surrounding the odontoid process: the crowned dens syndrome. Arthritis Rheum.1985;28(12):1417-1420.
2. Fenoy AJ, Menezes AH, Donovan KA, Kralik SF. Calcium pyrophosphate dehydrate crystal deposition in the craniovertebral junction. J Neurosurg Spine. 2008;8:22-29.
3. Siau K, Lee M, Laversuch CJ. Acute pseudogout of the neck—the crowned dens syndrome: 2 case reports and review of the literature. Rheumatol Int. 2011;31:85-88.
4. Aouba A, Vuillemin-Bodaghi V, Mutschler C, De Bandt M. Crowned dens syndrome misdiagnosed as polymyalgia rheumatica, giant cell arteritis, meningitis or spondylitis: an analysis of eight cases. Rheumatology. 2004;43:1508-1512.
Systemic Lupus Erythematosus
Germaine L. Defendi, MD
Olive View-University of California Los Angeles Medical Center
For 2 weeks, this 13-year-old girl felt tired and achy. She had persistent fevers (temperature up to 38.8°C [102°F]) and an erythematous facial rash above her eyebrows that extended to her cheeks and nasal bridge and spared the nasolabial folds. She had applied a topical acne medication to the rash but noted no improvement. She also reported decreased oral intake because of discomfort from palatal ulcers. She had no significant medical or family history.
Results of laboratory studies included a white blood cell (WBC) count of 3100/µL; hemoglobin, 10.3 g/dL; hematocrit, 31%; platelet count, 158,000/µL; blood urea nitrogen, 20 mg/dL; creatinine, 1.2 mg/dL; aspartate aminotransferase, 47 U/L (range, 0-35 U/L); alanine aminotransferase, 75 U/L (range, 1-30 U/L); antinuclear antibody (ANA) titer, 1:1280; C3, 32 mg/dL (range, 90-180 mg/dL); C4, 8 mg/dL (range, 16-47 mg/dL); complement CH50, less than 13 U/mL (range, 31-66 U/mL); direct Coombs IgG-positive, Smith antibodies indirect hemagglutination assay titer, 1:800; erythrocyte sedimentation rate, 45 mm/h (range, 0-20 mm/h). Routine urinalysis showed proteinuria (100 mg/dL), 15 WBCs, and 8 red blood cells, with moderate values for leukocyte esterase and blood. An echocardiogram showed normal valve function and no vegetations. An abdominal ultrasonogram revealed hepatomegaly.
 The patient was hospitalized, and the rheumatology team was consulted. Systemic lupus erythematosus (SLE) was diagnosed on the basis of the clinical history and physical findings, particularly the malar facial rash and oral ulcers. Laboratory studies supporting the diagnosis included the elevated ANA titer; hypocomplementemia; anemia; nephritis, with an elevated creatinine level for age; elevated levels of hepatic transanimases; the positive direct Coombs test result, reflective of a hemolytic process; and the presence of anti-Smith antibodies.1 After treatment with intravenous methylprednisolone sodium succinate, she clinically improved and was discharged.
The patient was hospitalized, and the rheumatology team was consulted. Systemic lupus erythematosus (SLE) was diagnosed on the basis of the clinical history and physical findings, particularly the malar facial rash and oral ulcers. Laboratory studies supporting the diagnosis included the elevated ANA titer; hypocomplementemia; anemia; nephritis, with an elevated creatinine level for age; elevated levels of hepatic transanimases; the positive direct Coombs test result, reflective of a hemolytic process; and the presence of anti-Smith antibodies.1 After treatment with intravenous methylprednisolone sodium succinate, she clinically improved and was discharged.
Her daily medications included prednisone, hydroxychloroquine, and an H2 blocker for gastric coverage while taking oral corticosteroids.2 Outpatient follow-up with rheumatology and ophthalmology were scheduled because of the increased risk of retinitis with use of hydroxychloroquine.3
Discussion. SLE (lupus) is a chronic autoimmune disorder characterized by multisystem microvascular inflammation, with the production of autoantibodies. Recurrent episodes of relapse and remittance occur. A defined cause is unknown. Factors involved in the development of SLE are race, genetics, hormonal changes, and the environment.4 The incidence in patients age 10 to 18 years varies among different populations; in the United States, it is highest among African Americans.5
As with other autoimmune diseases, females are affected more often than males. Onset of symptoms typically occurs after age 5 years; the incidence increases after age 10 years.1 Hormonal changes associated with puberty and pregnancy can trigger the disease.6 Genetic probability is increased in first-degree relatives with lupus and in identical twins.4
Commonly reported symptoms of lupus at initial presentation are fever, fatigue, and malaise of several months’ duration. Arthritis of the small joints in the hands and wrists and renal disease (nephritis or nephrosis) may manifest during this time.1 Presence of a malar rash is helpful for diagnosis; however, it occurs in only two-thirds of patients with SLE. The rash is usually a fixed (flat or raised) erythema that tends to spare the nasolabial folds. It can be painful or pruritic. Other cutaneous features are photosensitivity, a discoid rash that develops in sun-exposed areas (which may appear plaquelike with follicular plugging and scarring), and alopecia of the temporal regions.1 Hematological abnormalities of SLE are anemia, cytopenia, and thrombocytopenia.7 Associated cardiopulmonary conditions include pericarditis, endocarditis, coronary artery disease (early-onset atherosclerosis), and pleural disease.4

Neuropsychiatric manifestations (such as loss of academic performance, depression, and social isolation) can be indicators of SLE; thus, it is important to perform a workup for lupus in patients with isolated neuropsychiatric findings.8 More severe neurological presentations are seizures (20% of patients), and psychosis.9
Overall, the prognosis for patients with lupus is good. Poor outcomes are a result of limited access to healthcare and nonadherence to treatment regimens, which can lead to neurological complications, intercurrent infections, and extensive renal disease (such as diffuse proliferative glomerulonephritis).10 Survival rates are cited as 100% at 5 years and 85% at 10 years after diagnosis.11 ■
References:
1. Hiraki LT, Benseler SM, Tyrrell PN, et al. Clinical and laboratory characteristics and long-term outcome of pediatric systemic lupus erythematosus: a longitudinal study. J Pediatr. 2008;152:550-556.
2. Carreno L, Lopez-Longo FJ, Gonzalez CM, Monteagudo I. Treatment options for juvenile-onset systemic lupus erythematosus. Paediatr Drugs. 2002;4:241-256.
3. Bernstein HN. Ocular safety of hydroxychloroquine sulfate (Plaquenil). South Med J. 1992;85:274-279.
4. D’Cruz DP, Khamashta MA, Hughes GR. Systemic lupus erythematosus. Lancet. 2007;369:587-596.
5. Lim SS, Drenkard C, McCune WJ, et al. Population-based lupus registries: advancing our epidemiologic understanding. Arthritis Rheum. 2009;
61:1462-1466.
6. Costenbader KH, Feskanich D, Stampfer MJ, Karlson EW. Reproductive and menopausal factors and risk of systemic lupus erythematosus in women. Arthritis Rheum. 2007;56:1251-1262.
7. McNeil HP, Chesterman CN, Krilis SA. Immunology and clinical importance of antiphospholipid antibodies. Adv Immunol. 1991;49:193-280.
8. Brunner HI, Ruth NM, German A, et al. Initial validation of the Pediatric Automated Neuropsychological Assessment Metrics for childhood-onset systemic lupus erythematosus. Arthritis Rheum. 2007;57:1174-1182.
9. Steinlin MI, Blaser SI, Gilday DL, et al. Neurologic manifestations of pediatric systemic lupus erythematosus. Pediatr Neurol. 1995;13:191-197.
10. McCurdy DK, Lehman TJ, Bernstein B, et al. Lupus nephritis: prognostic factors in children. Pediatrics. 1992;89:240-246.
11. Ruperto N, Ravelli A, Cuttica R, et al; Pediatric Rheumatology International Trials Organization (PRINTO); Pediatric Rheumatology Collaborative Study Group (PRCSG). The Pediatric Rheumatology International Trials Organization criteria for the evaluation of response to therapy in juvenile systemic lupus erythematosus: prospective validation of the disease activity core set. Arthritis Rheum. 2005;52:2854-2864.
Rheumatoid Vasculitis
David I. Wolf, MD
Ten weeks before presentation, this 55-year-old woman noticed decreased sensation in her feet and a bluish discoloration of her toes. These symptoms progressed rapidly, and pain and coldness in both feet increased in intensity. Her feet subsequently became gangrenous. Her seropositive arthritis had been diagnosed about 6 years earlier. The disease had been well controlled until about 10 weeks before this photograph was taken. This image is a particularly good depiction of the livedo reticularis pattern involving the legs. The fishnet appearance of purple discoloration is frequently an indicator of vasculitis.

Rheumatoid vasculitis is a rare complication of rheumatoid disease and tends to affect patients with a long history of rheumatoid arthritis and a high rheumatoid factor titer. Most patients in this group would be expected to have rheumatoid nodules as well. Rheumatoid vasculitis may also cause hyperkeratotic papules around the elbows and knees, nail fold infarcts, deep cutaneous ulcers, and peripheral neuropathy or mononeuritis. ■
Heberden Nodes
Sonia Arunabh, MD
Bilateral swelling and pain in the distal interphalangeal (DIP) joints for several months brought this 65-year-old woman to her physician. She complained also of stiffness in the region of the DIP joints when she arose in the morning and after short periods (less than 15 minutes) of inactivity. A history such as this, in conjunction with the appearance of the patient’s hand, is typical of Heberden nodes, which are a manifestation of osteoarthritis (OA).

Initially, a single Heberden node usually appears; eventually, multiple nodes develop. Later, as OA progresses, Bouchard nodes are seen in the proximal interphalangeal joints. These nodes may be associated with little or no pain for long periods, and women are affected far more often than men. The altered digits may reveal other abnormalities, particularly fixed flexion deformities and radial or ulnar deviation at the DIP joint. Radiographic studies show narrowing of the joint space, subchondral sclerosis, and osteophyte formation. ■
Cough, Chest Pain, and Dyspnea in a Woman with Rheumatoid Arthritis
Navin M. Amin, MD
A 40-year-old Hispanic homemaker is admitted with a 3-week history of high fever, chest pain, and a dry, irritating cough. Her illness began insidiously with increasing right upper chest pain that is sharp, pleuritic, and rates a 6 on a pain scale of 1 to 10. The pain is associated with temperatures of up to 38.8°C (102°F) and chills, rigors, and profuse sweating that increase in the evening. Worsening dyspnea has been accompanied by a drop in effort tolerance.
The patient was seen at a local urgent care center and treated with levofloxacin for a week. A chest radiograph showed infiltrates in the right upper lobe. The symptoms worsened and the medication was switched to clarithromycin, but there was no marked improvement.

The patient has a history of rheumatoid arthritis (RA). Initially, she was treated with ibuprofen, then with corticosteroids and hydroxychloroquine. During the past 12 months, she has received a weekly injection of infliximab. No tuberculin skin test was done before the initiation of infliximab therapy because the patient told the rheumatologist that results of a tuberculin skin test the year before were negative.
The patient’s appetite is poor and she has lost 6 lb in the past 3 weeks. She denies hemoptysis, palpitations, ankle edema, lymphadenopathy, rash, and joint swelling. She has no history of nausea, vomiting, diarrhea, abdominal pain, jaundice, hematemesis, melena, headache, vision problems, seizures, syncope, weakness, paresthesias, urinary symptoms, or bleeding diathesis.
Both of her parents have type 2 diabetes; a younger brother has bronchial asthma. The patient smokes half a pack of cigarettes a day; she does not drink alcohol or use illicit drugs. She is sexually monogamous. She visited her grandparents in Mexico for 2 weeks a year ago.
Physical exam. This thin woman appears chronically ill. Her hands show changes consistent with chronic RA, including swan-neck deformity.
Heart rate is 122 beats per minute and regular; temperature, 38.8°C (102°F); respiration rate, 24 breaths per minute; blood pressure, 118/68 mm Hg. Her weight is 104 lb. Hydration status is good. Examination of the head and neck shows no icterus, erythema, or evidence of candidal infection. The mucosa and skin are pale; there are no rashes or tattoos. There is no palpable lymphadenopathy or ankle edema; the thyroid is not palpable. Chest movements are symmetric and equal bilaterally. The trachea is centrally located and the chest is resonant to percussion. Breath sounds are harsh in the right upper zone and coarse rales are heard. The jugular venous pressure and heart sounds are normal. The abdomen is soft and nontender with no organomegaly or fluid. Results of a neurologic examination are normal.
Laboratory tests. White blood cell count, 12,800/µL, with 80% polymorphonuclear leukocytes and 20% lymphocytes. Hemoglobin level, 10.2 g/dL; platelet count, 156,000/µL. A peripheral smear shows normocytic normochromic anemia. Erythrocyte sedimentation rate, 124 mm/h. Urinalysis results are normal. Blood glucose level, 92 mg/dL; blood urea nitrogen, 12 mg/dL; creatinine, 0.8 mg/dL; serum sodium, 138 mEq/L; potassium, 4 mEq/L; chloride, 100 mEq/L. Total bilirubin, 1 mg/dL; conjugated bilirubin, 0.6 mg/dL. Total protein, 7.8 g/dL; albumin, 3.2 g/dL; alkaline phosphatase, 118 U/L; aspartate aminotransferase, 24 U/L; alanine aminotransferase, 21 U/L. Two blood cultures are negative for organisms. Serologic evaluation for Coccidioides yields negative results. Serum ferritin, 350 ng/mL. Serum iron, 38 µg/dL. Total iron-binding capacity, 200 µg/dL.
A chest radiograph and sputum evaluation for acid-fast bacteria (AFB) are ordered.
Discussion. Rheumatoid disease progression involves high concentrations of tumor necrosis factor (TNF), the central component in the cascade of cytokines induced in RA that stimulates production of additional inflammatory mediators such as chemokines, prostaglandins, proteases, and growth factors that activate neutrophils, B cells, and endothelial cells.
The TNF inhibitors infliximab, etanercept, and adalimumab are widely used to reduce the erosive damage of RA. Neutralization of TNF significantly suppresses the immune response.
Clinical manifestations. Extrapulmonary presentations, which have been reported in 30% to 50% of cases, include fever of unknown origin, miliary tuberculosis (TB), TB-associated lymphadenopathy, peritonitis, enteritis, meningitis, and vertebral and bladder disease.
Pulmonary manifestations usually consist of chronic productive cough, hemoptysis, pleuritic chest pain, and dyspnea associated with constitutional symptoms such as fever, night sweats, lack of energy, and weight loss.
Diagnosis and treatment. A high index of suspicion is confirmed by demonstration of AFB either in biopsy material or sputum, in conjunction with sputum culture. Chest radiography or CT can be helpful.
Once the diagnosis is established, prompt and aggressive therapy is started with isoniazid, rifampin, ethambutol, and pyrazinamide. The regimen is continued for 2 months, followed by isoniazid and rifampin therapy for an additional 7 to 10 months. ■
1. American Thoracic Society, Centers for Disease Control and Prevention. Targeted tuberculin testing and treatment of latent tuberculosis infection. Am J Respir Crit Care Med. 2000;161:221-247.