
Starting Or Intensifying Insulin Therapy In Type 2 Diabetes: Challenges And Opportunities In Primary Care
ABSTRACT: Primary care providers (PCPs) must increasingly bear the burden that the global epidemic of type 2 diabetes mellitus (T2DM) represents. Insulin therapy is well-established as an initial treatment for T2DM, but patients with T2DM and their PCPs are often reluctant to introduce insulin therapy. The authors use patient cases to highlight the proper place for insulin therapy in managing T2DM. They also identify barriers to starting patients with T2DM on insulin, particularly in the primary care setting, and review solutions for overcoming those barriers. Education and training are effective tools for enabling many patients to manage their disease successfully. Providers can adopt practical algorithms to start patients on insulin therapy sooner after a diabetes diagnosis and to avoid unnecessary delays in intensifying therapy. Nurse practitioners and other allied healthcare professionals can be enlisted to help with treating and training patients with T2DM.
Type 2 diabetes mellitus (T2DM) is a global health problem, and primary care providers (PCPs) are increasingly responsible for managing a growing number of patients with T2DM.1,2 Medical training has provided PCPs with an understanding of how beta cells function in the pancreas, the mechanism of insulin resistance, and the relationship between genetic factors and the diagnosis and treatment of T2DM. PCPs who treat several members of a single family over time may have a unique opportunity to educate patients with apparent genetic and environmental risk factors for T2DM on how to prevent or delay the onset of diabetes.
Initial treatment of T2DM begins with lifestyle changes, such as encouraging patients to improve their diet and increase their level of physical activity in an effort to achieve a normal body mass index (BMI) and overcome insulin resistance. If lifestyle changes are unsuccessful, either because the patient cannot adhere to them or because insulin resistance persists, or if a patient presents with more advanced disease, it may be necessary to prescribe oral or injectable pharmacological therapies as appropriate.3 Injectable therapies, including insulin, are being used earlier in the treatment of T2DM as newer agents have become available that have more predictable side effects, result in less weight gain, and are less likely to cause hypoglycemia. Today, starting insulin early after diagnosis is an appropriate treatment strategy for many patients with T2DM. Thus, it is vital for every PCP to know when and how to initiate insulin therapy and, subsequently, how to intensify insulin therapy if necessary. It is also important to educate patients with T2DM about the possibility of using insulin early on so that they develop realistic expectations about treatment.4
CASE PRESENTATIONS
The following 2 cases highlight the place for insulin therapy in managing patients with T2DM. This clinical perspective enables a better understanding of the barriers to insulin therapy in the primary care setting and equally, how these might be overcome. Certainly, when conversing about the how-tos of initiating and intensifying insulin therapy, clinical analysis is a vital part of the dialogue.
CASE 1
A 56-year-old man presented to PCP for a routine checkup, reporting an increase in appetite and fatigue over the past 3 months, along with a higher frequency of urination. Despite a 35-pound weight gain during the past 3 years, he had lost 10 pounds in the past 3 months. At the time of his checkup, his BMI was 37 kg/m2 (up from 33 kg/m2 recorded at a checkup 1 year earlier) and his waist circumference was 44 inches. Other than increased abdominal girth, the findings of his physical examination were unremarkable and he showed no signs of microvascular or macrovascular complications. Blood pressure was 139/88 mm Hg.
At the patient’s checkup the previous year, lifestyle changes were recommended based on the results of his physical examination and laboratory tests and his family history of T2DM. However, between the 2 visits, his fasting plasma glucose (FPG) level increased from 122 mg/dL to 275 mg/dL. His presenting FPG, along with his current hemoglobin (HbA1c) level of 9.8%, indicated hyperglycemia. Changes in his lipid levels showed escalating dyslipidemia: his total cholesterol level increased from 200 mg/dL to 220 mg/dL; his triglyceride level increased from 200 mg/dL to 350 mg/dL; his high-density lipoprotein (HDL) level decreased from 38 mg/dL to 33 mg/dL; and his low-density lipoprotein level decreased from 122 mg/dL to 117 mg/dL. Patient reported a good social support system and adequate health insurance coverage.
• How would you treat a patient’s hyperglycemia?
Although lifestyle changes were discussed with the patient at his previous checkup, whatever changes he made failed to keep his condition from progressing. The combination of being genetically predisposed to T2DM and being obese appeared to have accelerated his insulin resistance and beta cell failure to where pharmacological intervention was critical to manage his hyperglycemia. To reduce the risk of developing microvascular and macrovascular complications, the patient needed to understand how imperative it was for him to continue making those lifestyle changes.
Patient’s presenting HbA1c of 9.8% was associated with significant glucotoxicity and needed to be lowered to a near-normal level (ie, <6.5%) as quickly as possible to reduce the toxic effects of excess glucose on his pancreas, thereby improving insulin sensitivity and beta cell function.5,6 Oral antidiabetes drugs (OADs) are less effective when HbA1c levels are as high as the patient’s were therefore not the best treatment option for him.
Several studies have shown that short-term intensive insulin therapy is effective at rapidly reinstating euglycemic conditions.6-8 In these studies, several daily injections of insulin for 2 to 3 weeks resulted in euglycemia.6-8 Roughly half the patients maintained euglycemia with diet alone or with OADs for at least 1 year after stopping insulin therapy. Basal insulin is an ideal initial therapy for reducing patient's FPG and HbA1c. It can be started at a low dose (eg, 10 U of long-acting analog insulin) administered each evening. The dose can be increased by 2 U to 3 U every third day as necessary if the patient’s average FPG is ≥140 mg/dL.9 In Case 1, it was evident that the patient would probably also need short-acting bolus insulin to reduce his postprandial blood glucose levels.
The patient’s dyslipidemia was also a concern. In addition to the triglyceride/HDL ratio being a risk predictor for coronary artery disease, a triglyceride/HDL ratio of >3 is a risk factor for insulin resistance.10 Patient had a high triglyceride/HDL ratio at his checkup 1 year earlier, which was worse at his most recent visit. This ratio, when considered with his risk factors of obesity and a family history of T2DM, suggested that he had prediabetes or possibly even diabetes. Tracking changes in a patient’s triglyceride/HDL ratio over time may indicate whether the patient has any improvement or deterioration in insulin resistance or sensitivity.
The extent to which the patient was able to recover from the double-edged insult of glucotoxicity and lipotoxicity partly depended on the duration of both conditions.5 He showed no signs of microvascular or macrovascular disease, which suggested his hyperglycemia and dyslipidemia were unlikely to have persisted long enough to cause extensive damage to other tissues and organs that might limit his recovery. Having a good social support system increased the likelihood that potentially fatal hypoglycemic episodes would go unnoticed, and having adequate health insurance meant his choice of therapy was unlikely to be limited by cost.
This case illustrates how hyperglycemia and dyslipidemia can escalate in a patient with T2DM risk factors (eg, obesity, a family history of T2DM, and dyslipidemia) and highlights possible indicators of disease progression that should not be overlooked. Had the physician taken a more aggressive approach to managing the patient's care in response to findings from the previous year’s checkup, it could have delayed his progression to T2DM.
 WHY PATIENTS AND PRIMARY CARE PROVIDERS OFTEN DELAY INSULIN THERAPY
WHY PATIENTS AND PRIMARY CARE PROVIDERS OFTEN DELAY INSULIN THERAPY
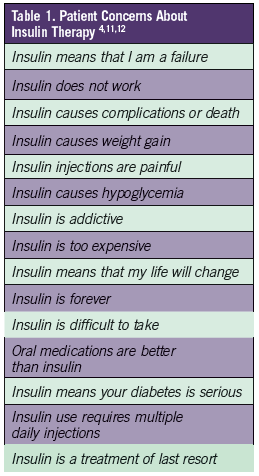
Concerns of patients and their PCP may lead to a delay in starting insulin therapy. A combination of real issues and unfounded or outdated beliefs about insulin therapy may be behind patients’ reluctance to start insulin therapy (Table 1).4,11,12Targeted patient education can help address many of these concerns. The primary reason patients hesitate to start insulin is because they believe it means they have failed. To prevent or correct patients’ misperception that starting insulin represents a personal failure, PCPs should discuss the pathophysiology of beta cell decline; explain the stages of treatment, including insulin, at the time of diagnosis; and assure patients they are not to blame. Many patients associate insulin with poor outcomes, such as dialysis, amputation, or early death. Education can help patients understand that early use of insulin does not increase the risk of serious morbidities associated with advanced T2DM and may even prevent them.4,11,12
When it comes to starting patients on insulin therapy, many PCPs suffer from clinical inertia, which is the failure to initiate or intensify therapy when indicated.13 A survey of Japanese physicians underscored the role of clinical inertia in delaying insulin treatment for patients with T2DM.14 Physicians who were surveyed identified an HbA1c of 8.2% as the threshold at which they would consider taking insulin if they had T2DM, whereas an HbA1c of 8.7% was the threshold at which the physicians said they would consider starting their patients with T2DM on insulin; the mean HbA1c level at which the physicians actually recommended insulin therapy for their patients was 9.6%. Clinical inertia may result from various real and perceived concerns, including:1,2,4,15,16
• Concern that hypoglycemia may compromise patient safety
• Belief that insulin therapy is not cost-effective and should be delayed as long as possible
• Perception that insulin therapy places a greater burden on resources (time and cost) and is too complex to be managed in a busy primary care practice
• Lack of confidence in patients’ ability to understand and manage insulin therapy and that this might result in treatment nonadherence
• Presumption that the patient will be unwilling or unable to inject themselves with insulin
• Concern that insulin therapy will degrade the patient’s quality of life
• Uncertainty regarding the initial dosing and titration of insulin due to the manufacturer’s vague prescribing information.
EASING THE BURDEN OF INSULIN THERAPY ON PRIMARY CARE
To select an appropriate insulin regimen and provide tailored patient education, PCPs need to understand the benefits of insulin therapy and gain familiarity with available self-management programs. It is also important for PCPs to stay abreast of current treatment guidelines for T2DM, particularly regarding the roles of early insulin therapy and newer antidiabetic agents. More practical guidance than ever before is readily available on tailoring therapy for individual patients.4
Resources are also available to help overcome practical concerns, such as how to facilitate insulin therapy for T2DM patients in the setting of a busy primary care practice. It would prove beneficial for PCPs treating these patients to expand the roles of office nurses, medical assistants, nurse practitioners, and physician assistants, and to increase referrals to diabetes educators (nurses, dieticians, and pharmacists) and diabetes education programs.
• Self-management programs.
Self-management programs empower patients to take control of the daily management of their disease, allowing them to manage their blood glucose levels safely and effectively. Most patients can achieve optimum glycemic control as long as they receive appropriate instructions on self-titration.17In addition, by helping patients manage their own insulin therapy, these programs can ease the burden on the busy PCP.
Numerous examples of patient-driven titration algorithms are available, some of which will be discussed later in this article.18,19 For example, the self-management program outlined by Harris and colleagues18 on the use of bolus insulin at breakfast in patients already using basal insulin was recently found to be simple, safe, and effective; the program improved glycemic outcomes without causing severe hypoglycemia.
A pooled analysis of data from patients with T2DM who were randomly assigned to 1 of 3 regimens based on insulin with insulin glargine for 24 weeks showed a 1.4% to 1.8% reduction in HbA1c levels and low rates of hypoglycemia.19 The 3 self-titration algorithms used in the study were (1) insulin glargine increased by 1 U once daily if average FPG was >100 mg/dL; (2) insulin glargine increased by 2 U every 3 days if average FPG was >100 mg/dL; and (3) a treat-to-target approach in which insulin glargine was increased by 2 U to 8 U weekly based on 2-day mean FPG levels. All 3 algorithms resulted in similar levels of glycemic control, but algorithms 1 and 2 were associated with less hypoglycemia.
• Referrals to diabetes educators.
It is critically important for PCPs at all levels to stress the importance of diabetes education. Diabetes educators, nurse practitioners, and others with advanced training in diabetes can be instrumental in improving diabetes management in the primary care setting.20 These experts can provide crucial education and support and help monitor patients undergoing intensification of insulin therapy.
Many primary care offices do not employ registered nurses, dietitians, or certified diabetes nurse practitioners, so it may be necessary to identify community resources for referral purposes. Improving integration of the healthcare system’s public and private sectors, using multidisciplinary teams, and possibly involving the pharmaceutical industry (with appropriate regulation) may be important components for improving successful initiation of insulin therapy.21 PCPs can contribute to the discussion by highlighting the lack of supportive resources for patients starting injectable medications and by stressing the need for patients to have access to diabetes nurse practitioners. Other options to help patients start insulin include diabetes group visits and simple phone calls to patients from office support staff to provide self-management suggestions.22,23Ongoing family and social support are critical in helping patients sustain insulin therapy.
INITIAL INSULIN THERAPY
• When to start insulin.
Insulin therapy should be strongly considered as the primary treatment for patients who have significant hyperglycemic symptoms and a dramatically elevated plasma glucose concentration (eg, >300-350 mg/dL) or HbA1c level (eg, ≥10%-12%). Insulin therapy is mandatory for patients with catabolic features or ketonuria, which suggests the patient has profound insulin deficiency.24 More specific signs that insulin therapy should be started include symptoms of poor glucose control, such as nocturia, vaginitis, fatigue, or sudden weight loss; suboptimal glycemic control (HbA1c level, 7%-10%) for at least 4 months despite high doses of OADs; and frequent HbA1c levels above 8%.9 Insulin therapy should also be considered for informed motivated patients who believe their treatment goals are not being met.
• When to stop insulin.
Insulin therapy may be stopped once hyperglycemia symptoms have subsided, glucotoxicity has resolved, the patient’s metabolic state has stabilized, and treatment goals have been achieved. The time it takes to achieve a stable metabolic state varies between patients, so setting a specific timeframe for insulin use is not possible. It is better to let each patient’s individual response serve as a guide for how long insulin therapy should be continued. Consider weaning patients off of insulin or stopping insulin when they have achieved their target glucose and HbA1c levels.
• Setting and achieving therapeutic goals.
The primary goal of therapy is to maintain HbA1c levels at <6.5% to 7.0%, while minimizing therapy’s adverse effects, such as weight gain and hypoglycemia. For patients who have risk factors such as reduced life expectancy, minimal support, diabetes for a longer duration, and significant morbidity, the HbA1c goal may be less stringent and closer to 8.0%.3
The appropriate insulin dose can be selected once the target HbA1c level has been set; initial daily insulin doses are typically low (eg, 0.1-0.2 U/kg), but they may be higher (0.3-0.4 U/kg) if hyperglycemia is severe or insulin resistance is high. A convenient starting regimen for insulin therapy is a single injection of basal insulin, timed according to the patient’s schedule and overall glucose profile. Noninsulin agents may be continued with basal insulin, but insulin secretagogues (ie, sulfonylureas or meglitinides) typically should be discontinued as the insulin regimen becomes more complex.
Because months may elapse between clinic appointments and patients with persistent hyperglycemia need prompt intervention, consider providing motivated patients capable of self-adjusting their medication with insulin intensification schedules. Persistent hyperglycemia indicates the need for a small dose increase, and several algorithms are available for enabling patients to titrate their insulin dose.3 A reasonable titration approach is to add 1 U to 2 U of insulin to the daily dose (or increase an already high dose by 5% to 10%) once or twice weekly if the FPG level exceeds the specified target, which is usually 130 mg/dL to 140 mg/dL. As the FPG level comes closer to the targeted level, dose adjustments should be smaller and less frequent. An example of a treat-to-target algorithm is shown in Table 2.9

• Choice of basal insulin.
Suitable basal insulins for patients starting insulin therapy include neutral protamine Hagedorn (NPH), an intermediate-acting human insulin; or a long-acting insulin analogs, such as insulin glargine or insulin detemir.3,25 Treatment selection should consider the advantages and disadvantages of each type of basal insulin3,9,25 and each patient’s needs and characteristics. Factors to consider when choosing a basal insulin formulation include the drug’s effectiveness at reducing glucose levels, extra-glycemic effects with the potential to reduce long-term complications, its safety and tolerability profiles, ease of use, and cost.26
A basal-only insulin regimen carries a lower risk of hypoglycemia and weight gain than premixed insulin regimens. Long-acting analogs are preferred over NPH because they are associated with a lower incidence of overnight hypoglycemia. Insulin glargine and insulin detemir are also available in pen form, whereas NPH is only available in vials. Many patients prefer insulin pens, which are more convenient and easier to use than a vial and syringe. Insulin pens may also provide more accurate dosing for patients who have functional or visual impairment. However, NPH therapy tends to cost less and, depending on other considerations, may be a better option than insulin glargine or insulin detemir for patients for whom cost is a concern. In weighing financial “cost,” consideration should be given to the cost implications of adverse effects, additional monitoring requirements, and the risk of long-term complications.24
(Case 2 and Intensifying Insulin Therapy on next page)
INTENSIFYING INSULIN THERAPY
When basal insulin therapy alone fails to provide overall glycemic control, therapy should be intensified to improve postprandial glucose control. Algorithms are available for tailoring decisions about intensifying insulin therapy to individual patients.27 Options for achieving postprandial glycemic control include rapid-acting insulin analogs, premixed insulins, and incretins. As always, each option has disadvantages and advantages.
It is easy to add rapid-acting insulin analogs (eg, aspart, lispro, and glulisine) and regular insulin to a basal insulin regimen—administered as a supplement before meals—to create a basal-bolus approach, but 1 disadvantage is that multiple bolus doses may be needed to achieve targets.27 Adding a second or third bolus dose to achieve a full basal-bolus regimen can provide good glycemic control but can also cause hypoglycemia.
Premixed insulins, typically administered twice daily, are a common alternative to the basal-bolus approach.27 At initial doses, this approach is more convenient and less likely to cause hypoglycemia than the basal-bolus approach. To provide a level of glycemic control similar to that provided by the basal-bolus approach, therapy with premixed insulins can be intensified by adding a midday bolus dose, but this may increase the risk of hypoglycemia and weight gain.
Incretins (ie, glucagon-like peptide-1 receptor agonists and dipeptidyl peptidase-4 inhibitors) can be added to basal insulin therapy without increasing the risk of hypoglycemia. This approach has the benefit of being weight-neutral or even resulting in weight loss.28 However, incretins may cause nausea and vomiting in some people.27
PATIENT STATUS AND TREATMENT CHOICES
The patient’s overall health status, including age, comorbidities, and degree of frailty, should be taken into account when setting glycemic targets and making treatment choices. Patients 65 years and older may have a higher atherosclerotic disease burden, reduced renal function, and additional comorbidities. Those patients taking other medications for a comorbid condition are at greater risk of experiencing treatment-related adverse events and drug-drug interactions. In older patients, unsteadiness due to hypoglycemia may result in falls and fractures. Life expectancy may also be reduced.24 Some patients may be socially and economically disadvantaged, which are important considerations when selecting treatment.
Glycemic targets for patients who are frail or elderly or who have comorbidities or reduced life expectancy may need to be less stringent. For example, an HbA1c target of <7.5% to 8.0% may be more acceptable. When choosing an antihyperglycemic agent, safety and avoiding hypoglycemia are paramount concerns. But the potential effects of the drug on conditions such as heart failure, renal dysfunction, fracture risk, and possible drug-drug interactions should also be considered.
CASE 2
Case 2 illustrates the importance of setting individualized HbA1c targets for patients, as recommended in guidelines issued jointly by the European Association for the Study of Diabetes and the American Diabetes Association.3 This second patient, a 78-year-old man, had been living with T2DM for a long time before presenting with renal insufficiency, hypertension, hyperlipidemia, and coronary artery disease. History intake revealed daily, evening doses of several OADs and 25 U of basal insulin. Additionally, patient admitted to a pattern of skipping meals, which has resulted in several episodes of hypoglycemia. His morning glucose readings are usually <140 mg/dL; his bedtime readings are higher if he eats supper late. His most recent HbA1c measurement was 7.2%. Due to the patient’s advanced age and comorbid conditions, combined with the fact that he lives alone and experiences potentially life-threatening hypoglycemic events, a less stringent HbA1c target of <8.0% would be appropriate and more manageable.
CONCLUSION
The role of using insulin early in the treatment of T2DM is well-established. It is important to recognize patient and PCP-related barriers to starting insulin therapy. Targeted education is effective in overcoming many patient barriers. To reduce the burden of T2DM in the primary care setting, self-management programs can be used to education patients on how to titrate their diabetes medications. By staying up-to-date with current guidelines on insulin use and following practical algorithms on initiating and titrating therapy, busy PCPs can facilitate earlier insulin use and avoid unnecessary delays in intensifying therapy for their T2DM patients. Whenever possible, assistance should be sought from diabetes educators, nurse practitioners, and other healthcare professionals trained to help patients manage diabetes.
The authors of this manuscript have elected to not receive the honorarium offered by Consultant for publication of this article in the journal.
Ed Shahady, MD, is medical director diabetes Master Clinician Program in Fernandina Beach, FL.
Jane F. Kapustin, is with the University of Maryland School of Nursing in Baltimore, MD.
Theresa McGhee, is with AbsoluteCARE Medical Center in Atlanta, GA.
ACKNOWLEDGMENTS
The contents of the paper and the opinions expressed within are those of the authors, and it was the decision of the authors to submit the manuscript for publication. The authors contributed to the writing of this manuscript, including critical review and editing of each draft, and approval of the submitted version. The authors received writing/editorial support in the preparation of this manuscript provided by Rosalie Gadiot, PhD, of Excerpta Medica, funded by Sanofi US, Inc.
References:
1.Philis-Tsimikas A. Initiating basal insulin therapy in type 2 diabetes: practical steps to optimize glycemic control. Am J Med. 2013;126(9 suppl 1):S21-S27.
2.Arnolds S, Heise T, Flacke F, Sieber J. Common standards of basal insulin titration in type 2 diabetes. J Diabetes Sci Technol. 2013;7(3):771-788.
3.Inzucchi SE, Bergenstal RM, Buse JB, et al. Management of hyperglycemia in type 2 diabetes: a patient-centered approach: position statement of the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care. 2012;35(6):1364-1379.
4. Meece J. Dispelling myths and removing barriers about insulin in type 2 diabetes. Diabetes Educ. 2006;32(1 suppl):9S-18S.
5. Gleason CE, Gonzalez M, Harmon JS, Robertson RP. Determinants of glucose toxicity and its reversibility in the pancreatic islet beta-cell line, HIT-T15. Am J Physiol Endocrinol Metab. 2000;279(5):E997-1002.
6. Li Y, Xu W, Liao Z, et al. Induction of long-term glycemic control in newly diagnosed type 2 diabetic patients is associated with improvement of beta-cell function. Diabetes Care. 2004;27(11):2597-2602.
7. Ilkova H, Glaser B, Tunçkale A, et al. Induction of long-term glycemic control in newly diagnosed type 2 diabetic patients by transient intensive insulin treatment. Diabetes Care. 1997;20(9):1353-1356.
8. Ryan EA, Imes S, Wallace C. Short-term intensive insulin therapy in newly diagnosed type 2 diabetes. Diabetes Care. 2004;27(5):1028-1032.
9. Spollett GR. Insulin initiation in type 2 diabetes: what are the treatment regimen options and how can we best help patients feel empowered? J Am Acad Nurse Pract. 2012;24(suppl 1):249-259.
10. Reaven G. Metabolic syndrome: pathophysiology and implications for management of cardiovascular disease. Circulation. 2002;106(3):286-288.
11. American Diabetes Association. Insulin myths and facts. http://clinical.diabetesjournals.org/content/25/1/39.full. Accessed February 2015.
12. Kunt T, Snoek FJ. Barriers to insulin initiation and intensification and how to overcome them. Int J Clin Pract Suppl. 2009;(164):6-10.
13. Phillips LS, Branch WT, Cook CB, et al. Clinical inertia. Ann Intern Med. 2001;135(9):825-834.
14. Ishii H, Iwamoto Y, Tajima N. An exploration of barriers to insulin initiation for physicians in Japan: findings from the Diabetes Attitudes, Wishes and Needs (DAWN) JAPAN Study. PLoS One. 2012;7(6):e36361.
15. Peyrot M, Rubin RR, Lauritzen T, et al. Resistance to insulin therapy among patients and providers: results of the cross-national Diabetes Attitudes, Wishes, and Needs (DAWN) study. Diabetes Care. 2005;28(11):2673-2679.
16. Reach G, Le Pautremat V, Gupta S. Determinants and consequences of insulin initiation for type 2 diabetes in France: analysis of the National Health and Wellness Survey. Patient Prefer Adherence. 2013;7:1007-1023.
17. Khunti K, Davies MJ, Kalra S. Self-titration of insulin in the management of people with type 2 diabetes: a practical solution to improve management in primary care. Diabetes Obes Metab. 2013:15(8):690-700.
18. Harris SB, Yale JF, Berard L, et al. Does a patient-managed insulin intensification strategy with insulin glargine and insulin glulisine provide similar glycemic control as a physician-managed strategy? Results of the START (Self-Titration with Apidra to Reach Target) Study: a randomized noninferiority trial. Diabetes Care. 2014;37(3):604-610.
19. Dailey G, Aurand L, Stewart J, et al. Comparison of three algorithms for initiation and titration of insulin glargine in insulin-naive patients with type 2 diabetes mellitus. J Diabetes. 2014;6(2):176-183.
20. Kruger DF. Intensifying insulin treatment: options, practical issues, and the role of the nurse practitioner. J Am Acad Nurse Pract. 2012;24(suppl 1):260-269.
21. Lee PY, Lee YK, Ng CJ. How can insulin initiation delivery in a dual-sector health system be optimised? A qualitative study on healthcare professionals’ views. BMC Public Health. 2012;12:313.
22. Shahady E. Group visits for diabetes: an innovative way to overcome barriers and achieve quality care. Consultant. 2010;50:480-486.
23. Shahady E. Disease registries and teamwork-keys to a patient centered medical home for diabetes. Practical Diabetology. 2010;29:20-25.
24. Inzucchi SE, Bergenstal RM, Buse JB, et al. Management of hyperglycaemia in type 2 diabetes: a patient-centered approach. Position statement of the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetologia. 2012;55(6):1577-1596.
25. Shubrook JH. Insulin for type 2 diabetes: how and when to get started. J Fam Pract. 2014;63(2):76-81.
26. Nathan DM, Buse JB, Davidson MB, et al. Medical management of hyperglycemia in type 2 diabetes: a consensus algorithm for the initiation and adjustment of therapy: a consensus statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care. 2009;32(1):193-203.
27. Meneghini LF. Intensifying insulin therapy: what options areavailable to patients with type 2 diabetes? Am J Med. 2013;126(9 suppl 1):S28-37.
28. Gerich, J. Pathogenesis and management of postprandial hyperglycemia: role of incretin-based therapies. Int J Gen Med. 2013;6:877-895.