
Rasmussen’s Aneurysm
A 49-year-old male presented to the emergency room with hemoptysis, coughing up 400 cc of bright red blood. He complained of the productive cough for the previous 6 months, and was treated for community-acquired pneumonia without resolution of his symptoms.
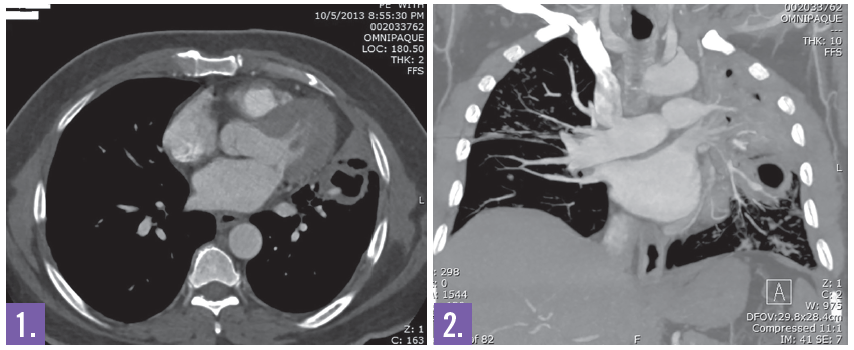
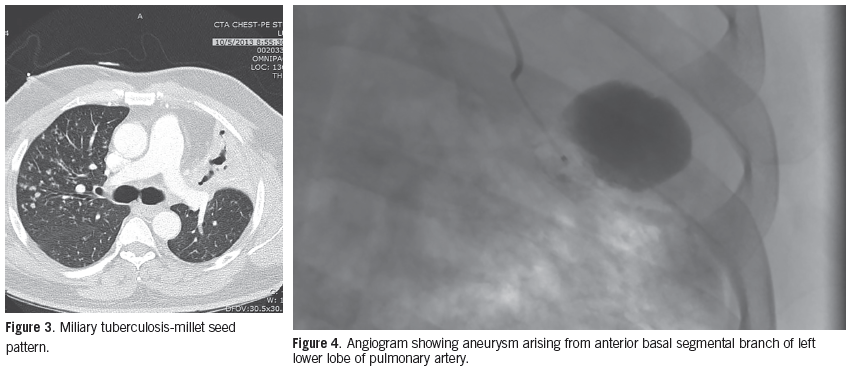
Diagnostic tests. Initial chest x-ray showed interstitial nodular densities and infiltrates throughout both lungs with consolidation, left moderate sized effusion, and decreased left lung volume with left sided mediastinal shift. The chest CT demonstrated a 6.3 cm left upper lobe cavitary lesion (Figures 1 and 2), 3.6 cm left lower lobe cavitary lesion, lingual and anteromedial left lower lobe bronchiectasis, and right upper lobe centrilobular nodules. Sputum was positive for acid-fast bacilli. The patient was diagnosed with active pulmonary tuberculosis (Figure 3).
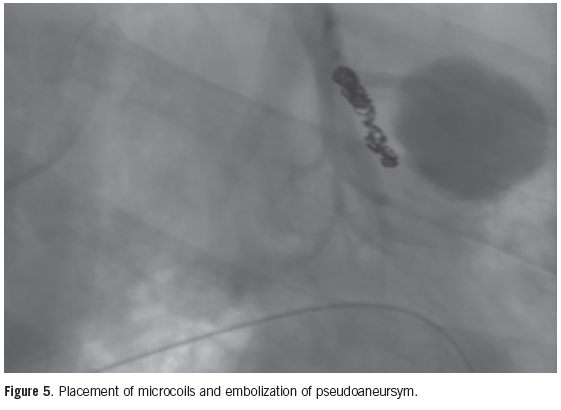
Treatment. He was started on a 4-drug regimen of isoniazid, ethambutol, pyrazinamide, and rifampin. On day 4 of his hospital stay, he had an unexpected massive hemoptysis and a subsequent cardiac arrest. Resuscitation was achieved and the patient underwent an emergent pulmonary artery angiography, which revealed active bleeding from a Rasmussen’s aneurysm arising from the anterior basal segmental branch of the left pulmonary artery (Figure 4). The vessel was successfully embolized utilizing microcoils (Figure 5).
Outcome of the case. The patient continued to be intubated and unresponsive with frequent myoclonic jerking. He later expired on day 5 of his hospital stay.
Discussion. Tuberculosis is a preventable cause of morbidity and mortality. A complication of pulmonary tuberculosis is Rasmussen’s aneurysm, which is caused by the erosion of an adjacent tuberculous cavity into the pulmonary artery.1,2 Tuberculous involvement of the pulmonary artery, along with local inflammation, weakens the arterial wall as granulation tissue replaces the adventia and the media. This is replaced by fibrin that causes thinning of the arterial wall and subsequent development of the aneurysm.3,4 It has a prevalence of 5%, and its rupture can lead to severe hemoptysis.3
Rasmussen’s aneurysm occur most frequently in chronic fibrocaseous tuberculosis and can develop despite appropriate antitubercular treatment.4 A fatal complication of pulmonary tuberculosis is massive hemoptysis due to the rupture of Rasmussen’s aneurysm, which has a mortality that is greater than 50%.3,5
Research. In a landmark study done by Auerbach in 1939, Rasmussen’s aneurysms were reported in 45 out of 1114 autopsies (4%) with chronic cavitary tuberculosis, of which 38 died due to rupture of the aneurysm.6 In a retrospective study by Khalil et al of 189 patients treated by endovascular means for severe hemoptysis, 13 had hemoptysis of pulmonary arterial origin, and 4 (2.1%) were due to active tuberculosis.7
Considering the life-threatening course of Rasmussen’s aneurysm rupture, various diagnostic measures have been explored. Bronchoscopy allows to localize the hemorrhage to a specific lobe, which helps to direct the angiographic evaluation.6 Chest CT with contrast that shows enhancing mass near an adjacent vessel can suggest Rasmussen’s aneurysm.1 Khalil et al found that multidetector row CT angiography (MDCTA) allow for the identification and early treatment of hemoptysis from pulmonary arterial origin.7 However, pulmonary angiography is required for the confirmation of the aneurysm.6 In a study by Sanyika et al, selective pulmonary angiography was performed on 8 patients with severe hemoptysis, of which 3 patients demonstrated Rasmussen’s aneurysm and were effectively treated.8 Shih et al found that the use of thoracic MDCTA and digital substrate angiography could differentiate between bleeding from pulmonary and bronchial origins.9
Treatment. The ideal management of severe hemoptysis is currently inconclusive. The indication for radiological or surgical intervention is considered when hemoptysis of >200 ml per 24 hours occurs.2 Surgical lobectomy provides a definitive treatment when the bleeding can be localized to a single lobe and the patient is operable, but has a postoperative complication rate of 50% and a mortality of 20%.3,10 Pulmonary arterial embolization is considered a first-line treatment for major hemoptysis from a pulmonary source and when the patient is a poor surgical candidate.2,3 Detachable balloons and steel coils have been commonly used for embolization. Prophylactic embolization has been suggested for unruptured pulmonary aneurysms.8
References:
- Rasmussen aneurysms as a treatment of hemoptysis. Radiology. 1994;193(2):396-398.
- Jayet PY, Denys A, Zellweger JP, et al. Successful embolization of Rassmussen’s aneurysm for severe hemoptysis. Swiss Med Wkly. 2004;134(47-48):705-706.
- Wang W, Gao L, Wang X. Rasmussen’s aneurysm with aspergilloma in old, healed pulmonary tuberculosis. Clin Imaging. 2013;37(3):580-582.
- Gesuete V, Corzani A, Bronzetti G, Lovato L, Picchio FM. Rasmussen’s aneurysm in childhood: a case report. Congenit Heart Dis. 2013;8(2):E41-E44.
- Zhang Y, Chen C, Jian GN. Surgery of massive hemoptysis in pulmonary tuberculosis: immediate and long term outcomes. J Thorac Cardiovasc Surg. 2014;148(2):651-656.
- Hildebrandt JW, Tarver RD, Conces DJ Jr, Broderick LS, Patel NH. Diagnostic case study: rasmussen aneurysm. Semin Respir Infect. 1998;13(2):160-162.
- Khalil A, Parrot A, Nedelcu C, Fartoukh M, Marsault C, Carette MF. Severe hemoptysis of pulmonary arterial origin: signs and role of multidetector row CT angiography. Chest. 2008;133(1):212-219.
- Sanyika C, Corr P, Royston D, Blyth DF. Pulmonary angiography and embolization for severe hemoptysis due to cavitary pulmonary tuberculosis. Cardiovasc Intervent Radiol. 1999;22(6):457-460.
- Shih SH, Tsai IC, Chang YT, Tsan YT, Hu SY. Fatal haemoptysis cased by a ruptured Rasmussen’s aneurysm. Thorax. 2011;66(6):553-554.
- Keeling AN, Costello R, Lee MJ. Rasmussen’s aneurysm: a forgotten entity? Cardiovasc Intervent Radiol. 2008;31(1):196-200.