
Pulmonary Hamartoma
Authors:
Sudhakar Reddy Konda, MD; Padmini Gudibanda, MBBS; and Anuradha Kolluru, MD
Citation:
Konda SR, Gudibanda P, Kolluru A. Pulmonary hamartoma. 2015;55(9):756.
A 71-year-old female with no significant past medical history presented to the hospital with sudden onset of massive hemoptysis. She denied any constitutional symptoms prior to presentation, including weight loss, cough, or shortness of breath.
History. She had a 40-pack year history of smoking.
Physical examination. This revealed a regular tachycardia at 108 beats per minute and a blood pressure of 128/72 mm Hg. Chest and cardiovascular exam was essentially unremarkable.
Laboratory tests. Chest radiography revealed a well-circumscribed mass in the left lower lobe (Figure 1). Contrast enhanced CT of the chest revealed a well-defined mass, 5.4 cm in diameter in the left lower lobe, containing areas of attenuation suggestive of fat deposition—a characteristic of pulmonary hamartoma (Figure 2).

Figure 1. Left lower mass seen on chest radiograph.
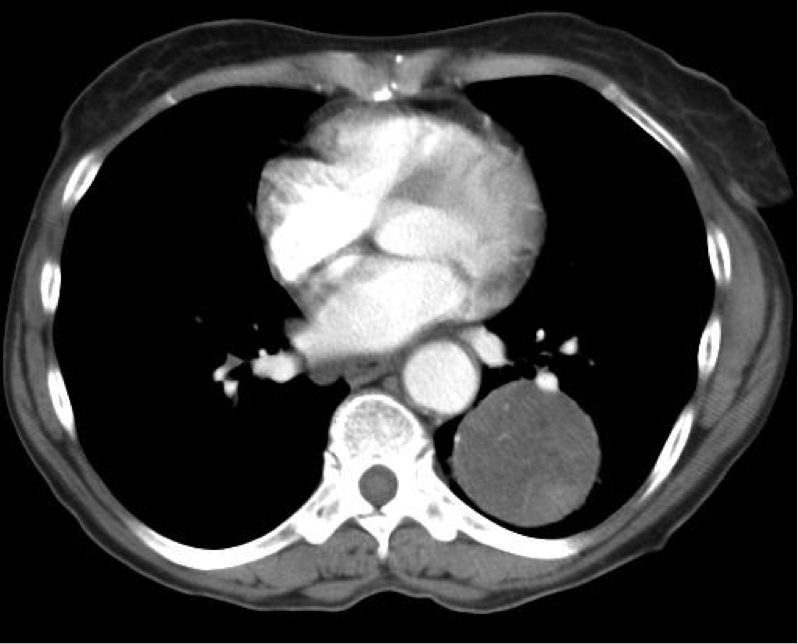
Figure 2. Contrast enhanced CT image of pulmonary hamartoma.
Fiber-optic bronchoscopy confirmed the mass as the source of bleeding. Therapeutic left lower lobectomy was performed and pathological examination was consistent with a pulmonary hamartoma.
Outcome of the case. One year later, she continues to do well with no recurrence of symptoms.
Discussion. Pulmonary hamartomas are benign, slow-growing tumors that account for 6% to 8% of all solitary pulmonary nodules.1 They are composed of tissues that are normally present in the lung, including fat, epithelial tissue, fibrous tissue, and cartilage. Pulmonary hamartomas have little or no malignant potential, and most of them are asymptomatic. However, because bronchogenic carcinoma is an important differential diagnosis,2 accurate imaging interpretation and diagnosis are important.3 Usually diagnosed as an incidental finding, these tumors are less likely to grow beyond 4 cm in diameter. They are very rarely known to cause hemoptysis and bronchial obstruction.
References:
- Hutter J, Reich-Weinberger S, Hutarew G, et al. Giant pulmonary hamartoma—a rare presentation of a common tumor. Ann Thorac Surg. 2006;82(2):e5-7.
- Jacob S, Mohapatra D, Verghese M. Massive chondroid hamartoma of the lung clinically masquerading as bronchogenic carcinoma. Indian J Pathol Microbiol. 2008;51(1):61-62.
- Zakharov V, Schinstine M. Hamartoma of the lung. Diagn Cytopathol. 2008;36(5):331-332.