
Pseudomonal Necrotizing Orchitis
A 65-year-old male presented with a 1-week history of left-sided testicular pain. His past medical history was significant for benign prostatic hypertrophy. The patient had an indwelling urinary catheter due to urinary retention. He had the catheter in place for 6 months and had it changed monthly by his urologist.
Physical examination. On initial exam, the left testicle was enlarged and extremely tender to palpation with a negative Prehn’s sign. Doppler ultrasound on admission showed a complex left hydrocele with internal echoes, along with mild scrotal wall thickening without evidence of testicular torsion. The patient was started on antibiotics.
RELATED CONTENT
Middle-Aged Man With Severe Upper Back and Neck Pain
Non-immunocompromised Pyomyositis
Laboratory results. Urology performed a needle decompression of the hydrocele; cultures from the drainage grew Pseudomonas aeruginosa. The patient was switched to cefepime (1 g IV q8h) and metronidazole (500 mg IV q8h) based on the culture sensitivities.
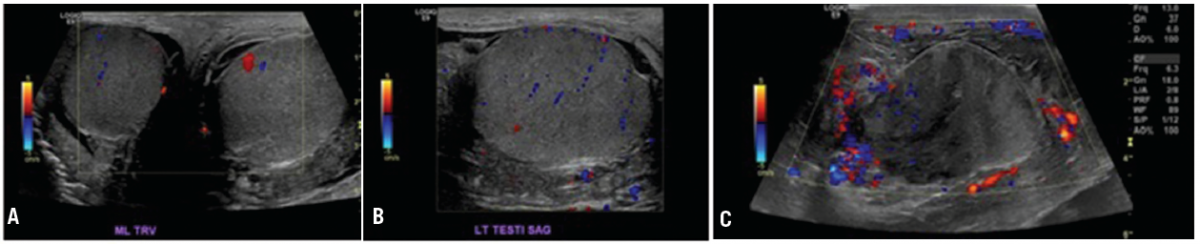
Figure 1. A. Ultrasound on admission showed an enlarged left testicle, hypoechoic left hydrocele, and mild left scrotal wall thickening with no evidence of torsion. B. Ultrasound on admission shows normal appearing left testicle with adjacent hydrocele. C. Repeat ultrasound 5 days after admission now showed hypoechoic areas within the left testicle.
Over the next few days, the patient reported no decrease in his pain. His leukocytosis worsened during his stay and he developed fevers. Ultrasound was repeated and changes were noted (Figure 1). There were new hypoechoic areas within the left testicle, and the hydrocele had more of a phlegmon-type appearance. A left scrotal exploration was done. A fair amount of phlegmon and fibrinous materials with a grossly abnormal appearance of the left testicle and epididymis was encountered.
A hydrocelectomy with excision of the sac and orchiectomy were performed and the specimens were sent to pathology. Scrotal fluid was sent to microbiology.
Treatment. Post surgery, the pathology reports were received. The first specimen showed a testicle with severe acute necrotizing orchitis. There was necrosis of the testis and epididymis with an edematous spermatic cord (Figure 2). The second specimen returned consistent with a hydrocele sac, also with necrosis. The cultures taken during surgery grew P aeruginosa.
In the days following surgery, the patient became afebrile and his pain resolved. He was able to tolerate oral feeding and was ambulating, so he was discharged home on day 10 of admission with ciprofloxacin (750 mg PO bid for 2 weeks) and metronidazole (500 mg PO q8h for 2 weeks) as well as outpatient follow-up with urology.
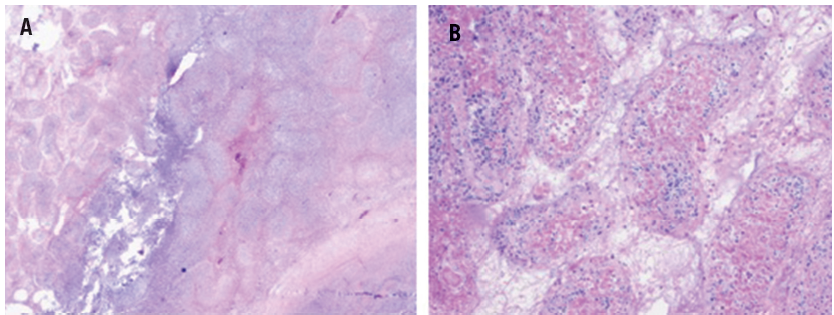
Figure 2. A. Low-powered image of left testicular seminiferous tubules shows necrosis with fibrosis, as well as a central abscess. B. High-powered image of the seminiferous tubule shows severely necrotic tissue with loss of nuclear stain.
Discussion. Isolated orchitis is extremely uncommon in adults and is usually accompanied by epididymitis, termed epididymoorchitis. Epididymitis is the most common cause of acute scrotal pain in adults. Most cases arise from infectious causes: most commonly Neisseria gonorrhoeae and Chlamydia trachomatis in patients under 35 years of age and gram-negative bacteria in older patients. C trachomatis has been estimated to make up 50% to 70% of acute cases with other causes; Mycobacterium tuberculosis, Escherichia coli, P aeruginosa, Treponema pallidum, Brucella species, and Ureaplasma species less frequently. From epididymitis, complications can arise including possible scrotal abscess and progression to epididymoorchitis.1
Epididymoorchitis often presents with unilateral, scrotal pain accompanied by high fevers, rigors, and possible swelling.1 The differential diagnosis includes testicular torsion, infection, hydrocele, varicocele, Fournier’s gangrene, trauma, and testicular cancer. Testicular torsion is a urologic emergency, so it is important to rule this out using a Doppler ultrasound.2 The urine analysis for these patients is often negative, so treatment is often started empirically.1
Recommended treatment includes ceftriaxone (250 mg IM single dose) followed by doxycycline (100 mg PO bid for 10 days) for C trachomatis and N gonorrhoeae coverage. Oral levofloxacin (500 mg PO daily for 10 days) can be added when gram-negative bacteria are suspected. If culture sensitivities return, the antibiotic regimen can be deescalated accordingly.1,3
Literature. After a thorough database search using Ovid Medline, PubMed, and UpToDate, multiple cases of epididymoorchitis were reviewed. A number of cases outlining severe epididymitis caused by Brucella species in Spain and Saudi Arabia were identified.4,5 Cases showing syphilis and tuberculosis as the causes were also found.2,6 One case of necrotizing epididymoorchitis in humans was identified without a published causative organism7 and one case of necrotizing epididymo-orchitis in rats caused by E coli.8 To our knowledge, this is the first case of necrotizing epididymoorchitis caused by P aeruginosa that has been published. ■
References:
1. Kasper DL, Braunwald E, Fauci AS, et al. Harrison's Principles of Internal Medicine. (17th ed.) New York: McGraw-Hill Medical Publishing Division; 2008.
2.D'Andrea A, Coppolino F, Cesarano E, et al. US in the assessment of acute scrotum. Crit Ultrasound J. 2013;5(suppl 1):S8.
3.Walker NA, Challacombe B. Managing epididymo-orchitis in general practice. Practitioner. 2013;257(1760):21-25.
4.González S, Encinas G, Napal L, et al. Brucellar orchiepididymitis with abscess. Arch Esp Urol. 1997;50(3):289-292.
5.Memish ZA, Venkatesh S. Brucellar epididymo-orchitis in Saudi Arabia: a retrospective study of 26 cases and review of the literature. BJU Int. 2001;88(1):72-76.
6.Sekita N, Nishikawa R, Fujimura M, et al. Syphilitic orchitis: a case report. Hinyokika Kiyo. 2012;58(1):53-55.
7.Muttarak M, Chiangmai W, Kitirattrakarn P. Necrotising epididymo-orchitis with scrotal abscess. BIIJ. 2005;1(2):e11.
8.Lu Y, Bhushan S, Tchatalbachev S, et al. Necrosis is the dominant cell death pathway in uropathogenic Escherichia coli elicited epididymo-orchitis and is responsible for damage of rat testis. PLoS One. 2013;8(1):e52919.