
The Potential Effect of Marijuana and Tobacco on Warfarin Metabolism and INR
AUTHORS:
Samarth P. Shah, PharmD, and Timothy H. Self, PharmD
CITATION:
Shah SP, Self TH. The potential effect of marijuana and tobacco on warfarin metabolism and INR. Consultant. 2016;56(12):1102-1103.
A patient’s response to warfarin is affected by several factors such as the use of other drugs, disease states, age, dietary vitamin K, and genetic poymorphisms.1,2 Due to its hepatic metabolism—most importantly, (S)-warfarin via the CYP2C9 isoenzyme of the cytochrome P450 system—this anticoagulant has numerous drug interactions that are essential to consider. In addition to the major pathway, warfarin is also metabolized by numerous minor pathways, CYP2C8, CYP2C18, CYP2C19, CYP1A2, and CYP3A4.1 Another key pharmacologic aspect of warfarin impacting its pharmacodynamic properties is that it is highly protein-bound.1 The therapeutic effectiveness of warfarin is measured by the international normalized ratio (INR). This review is focused on the effect of tobacco and marijuana on the response to warfarin.
Interaction With Marijuana
Marijuana has 4 major cannabinoid compounds, Δ9-tetrahydrocannabinol (THC), Δ8-THC, cannabinol, and cannabidiol.3,4 While the exact mechanism of the interaction between warfarin and marijuana is unknown, several theories have been proposed.
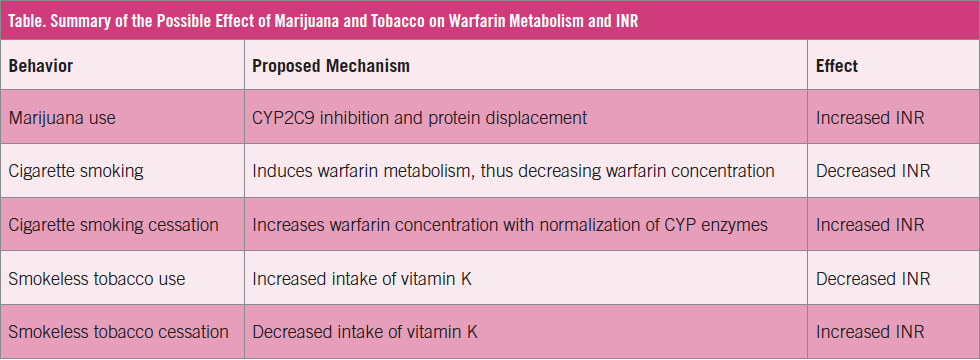
One theory centers on the interaction of metabolism within the cytochrome P450 system. One of the major cannabinoid compounds, cannabidiol, is known to be a weak inhibitor of CYP2C9, the major pathway for (S)-warfarin metabolism. Inhibition of this pathway can cause an increase in warfarin concentrations, thus leading to an increase in INR. Cannabidiol is also a potent inhibitor of CYP3A4. While CYP3A4 is described as a minor pathway for warfarin, inhibition of this pathway can also lead to an increased concentration of warfarin, thus leading to an increased INR.5,6
An alternative theory is based on the fact that warfarin and Δ9-THC are both highly plasma protein-bound.3,7 Accordingly, Δ9-THC has the potential to displace plasma protein-bound warfarin, thus leading to an increase in warfarin concentrations and an increased INR.3,7
Yamreudeewong and colleagues4 described a case depicting the impact of marijuana on a patient’s warfarin regimen. The patient had been on a stable warfarin dose for 11 years and was hospitalized for a gastrointestinal bleed. Five days before admission, the patient’s INR had been recorded as 3.2 at an anticoagulation clinic. At admission, his INR had increased to 10.4; after treatment, it dropped to 1.8 the next day. Fifteen days after discharge, the patient was readmitted, at which time his INR was 11.55, up from 1.94 as measured 6 days prior. At the time of this discharge, it had returned to 1.14. The patient described an increase in marijuana use from 1 g/wk to 2.5 g/wk throughout the period of the 2 admissions. Based on the Drug Interaction Probability Scale, the interaction was deemed to be probable. This case illustrates the importance of monitoring patients vigilantly if they are using marijuana while on warfarin therapy.
With the increasing number of states that have legalized marijuana and the number of patients who require warfarin therapy, this potential interaction clearly warrants more investigation and controlled studies.
Interaction With Cigarette Smoking
While there is a paucity of data to determine the clinical impact of smoking on warfarin, it is proposed that hydrocarbons in cigarette smoke induce CYP1A2, CYP1A1, and CYP2E1.8 The induction of these enzymes creates the potential for an increase in the concentration of warfarin, thus leading to an increase in INR. In addition, carbon monoxide may inhibit CYP enzymes,9 but very limited data are available to determine the clinical impact of these interactions. Initial publications have described no clinically significant difference in warfarin dosages between smokers and nonsmokers.8-11 However, one recent study found that smoking was associated with higher warfarin doses.12
Based on 3 published reports,9,13,14 managing a patient after smoking cessation may be clinically important. After stopping smoking, the induction of warfarin metabolism wanes, leading to an increase in warfarin concentration and an increase in INR. In a case reported by Evans and Lewis,9 a patient was on a warfarin dose of 58.75 mg/wk; after being stable for a month, his INR jumped to 5.5. The only change reported in this case was that the patient had stopped smoking tobacco. The patient was stable on the home dose for only a short time, and he had additional coagulopathies that could have impacted the warfarin response, but this case and 2 additional similar reported cases13,14 illustrate the importance of monitoring long-term smokers on warfarin therapy closely if they stop smoking.
Interaction With Smokeless Tobacco
Tobacco is rich in vitamin K1 (phylloquinone), which is found in green leafy vegetables.15 Ingestion of tobacco juice from smokeless or chewing tobacco thus is a significant source of vitamin K. A relatively large amount (1 kg) of smokeless tobacco ingestion is needed daily to surpass the recommended daily value of vitamin K.16 However, vitamin K is a fat-soluble vitamin, so it can accumulate in heavy users. Due to the increase in vitamin K intake, the effect of warfarin can be dampened, and the INR can decrease.
In a case reported by Kuykendall and colleagues,17 a patient in his 30s had used tobacco daily since the age of 12. He had been on long-term therapy with warfarin 25-30 mg/d, but over 4.5 years, his INR had never stabilized greater than 2.0. After a coagulopathy workup was negative, the patient decided to discontinue his tobacco use, and his INR increased from 1.1 to 2.3 within a week of quitting.
While minimal supporting evidence is available, patients with a heavy use of smokeless tobacco may have increased vitamin K intake and a reduced response to warfarin.
Key Points for Your Practice
Concomitant use of warfarin and marijuana or tobacco has the potential to cause serious harm and can result in hospitalization. Discussion of the use of any form of tobacco or marijuana should be discussed thoroughly with patients when managing their warfarin regimen. Due to the potential impact on INR, the use of marijuana or tobacco should not be taken lightly in patients who are receiving warfarin therapy. Practitioners should be vigilant in asking appropriate questions to ensure that patients are truthful about their use of marijuana and tobacco so that appropriate steps can be taken to ensure their anticoagulation plans are adjusted accordingly.
Samarth P. Shah, PharmD, is a postgraduate year 2 internal medicine pharmacy resident at the University of Tennessee Health Science Center and Methodist University Hospital in Memphis, Tennessee.
Timothy H. Self, PharmD, is a professor of clinical pharmacy at the University of Tennessee Health Science Center and the program director of the Postgraduate Year 2 Internal Medicine Pharmacy Residency at Methodist University Hospital in Memphis, Tennessee.
References:
- Ansell J, Hirsh J, Hylek E, Jacobson A, Crowther M, Palareti G. Pharmacology and management of the vitamin K antagonists: American College of Chest Physicians evidence-based clinical practice guidelines (8th edition). Chest. 2008;133(6 suppl):160S-198S.
- Self TH, Owens RE, Sakaan SA, Wallace JL, Sands CW, Howard-Thompson A. Effect of diseases on response to vitamin K antagonists. Curr Med Res Opin. 2016;32(4):613-620.
- Garrett ER, Hunt CA. Physicochemical properties, solubility, and protein binding of Δ9-tetrahydrocannabinol. J Pharm Sci. 1974;63(7):1056-1064.
- Yamreudeewong W, Wong HK, Brausch LM, Pulley KR. Probable interaction between warfarin and marijuana smoking. Ann Pharmacother. 2009;43(7):1347-1353.
- Bornheim LM, Everhart ET, Li J, Correia MA. Characterization of cannabidiol-mediated cytochrome P450 inactivation. Biochem Pharmacol. 1993;45(6):1323-1331.
- Sachse-Seeboth C, Pfeil J, Sehrt D, et al. Interindividual variation in the pharmacokinetics of Δ9-tetrahydrocannabinol as related to genetic polymorphisms in CYP2C9. Clin Pharmacol Ther. 2009;85(3):273-276.
- Widman M, Agurell S, Ehrnebo M, Jones G. Binding of (+)- and (–)-Δ1-tetrahydrocannabinols and (–)-7-hydroxy-Δ1-tetrahydrocannabinol to blood cells and plasma proteins in man. J Pharm Pharmacol. 1974;26(11):914-916.
- Garry J, Geraets DR. Effect of tobacco on INR. Am J Health Syst Pharm. 2007;64(8):804.
- Evans M, Lewis GM. Increase in international normalized ratio after smoking cessation in a patient receiving warfarin. Pharmacotherapy. 2005;25(11):1656-1659.
- Cropp JS, Bussey HI. A review of enzyme induction of warfarin metabolism with recommendations for patient management. Pharmacotherapy. 1997;17(5):917-928.
- Mitchell AA. Smoking and warfarin dosage. N Engl J Med. 1972;287(22):1153-1154.
- Shahin MHA, Khalifa SI, Gong Y, et al. Genetic and nongenetic factors associated with warfarin dose requirements in Egyptian patients. Pharmacogenet Genomics. 2011;21(3):130-135.
- Colucci VJ, Knapp JF. Increase in international normalized ratio associated with smoking cessation. Ann Pharmacother. 2001;35(3):385-386.
- Jordan SD, Stone MD, Alexander E, Haley J, McKee A. Patient case: impact of smoking cessation on international normalized ratio. J Pharm Pract. 2014;27(5):470-473.
- Olson R. Vitamin K. In: Shils ME, Olson JA, Shike M, eds. Modern Nutrition in Health and Disease. Vol 1. 8th ed. Philadelphia, PA: Lea & Febiger; 1994:342-357.
- Olsen JA. Recommended dietary intakes (RDI) of vitamin K in humans. Am J Clin Nutr. 1987;45(4):687-692.
- Kuykendall JR, Houle MD, Rhodes RS. Possible warfarin failure due to interaction with smokeless tobacco. Ann Pharmacother. 2004;38(4):595-597.