
Pneumocystis Pneumonia in a Boy With AIDS
Authors:
Roberto P. Santos, MD; Mary Ellen Adams, RN; and Martha L. Lepow, MD
Citation:
Santos RP, Adams ME, Lepow ML. Pneumocystis pneumonia in a boy with AIDS. Consultant. 2016;15(8).
A 17-year-old boy presented to the emergency department (ED) with a 3-day history of nonproductive cough, fever, and shortness of breath. The boy had a congenital HIV infection that had progressed to AIDS, with a low CD4+ T-lymphocyte count of 5 cells/mm3 (normal CD4, ≥ 500 cells/mm3). He also had a history of esophageal candidiasis and oral ulcers from herpes simplex virus 1. During the 3 years prior to presentation, the boy had not been taking combination antiretroviral therapy. In addition, the patient chose to discontinue prophylaxis for pneumocystis pneumonia (PCP).
When the boy arrived at the ED, his temperature was 37.7°C, his heart rate was 145 beats/min, his respiratory rate was 20 breaths/min, his blood pressure was 76/39 mm Hg, and he had oxygen saturation of 96% in room air. The boy was alert but was speaking in short sentences.
Examination results showed that he had oral thrush, tachycardia, and fine crackles through his lung fields. On admission, results of a chest radiograph showed right lower lobe consolidation that likely represented pneumonia (Figure 1). A complete blood count showed a white blood cell count of 9200 /µL, hemoglobin of 9.8 g/dL, a platelet count of 208 ×103/µL with a differential white blood cell count of 70% neutrophils, 13% bands, 10% monocytes, 4% lymphocytes, 1% atypical lymphocytes, and 1% eosinophils. Lactate dehydrogenase (LDH) was 353 U/L (reference range, 100-190 U/L), and blood cultures performed on admission showed no growth after 72 hours.
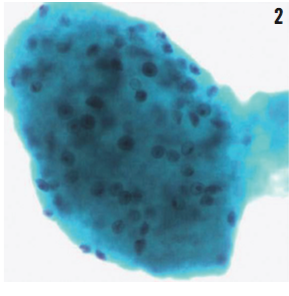
The boy was empirically started on intravenous ceftriaxone and moxifloxacin for community-acquired pneumonia and fluconazole for candida esophagitis. PCP prophylaxis was started, which consisted of trimethoprim-sulfamethoxazole (TMP-SMX) or TMP-SMX single strength, once daily. Combination antiretroviral therapy consisting of raltegravir, etravirine, and tenofovir-emtricitabine was also started. On day 1 from admission, a bronchoscopy was performed, and bronchoalveolar lavage specimens were sent for bacterial, fungal, and acid-fast bacilli cultures. All culture results were negative, though the bronchoalveolar lavage specimen showed an increased number of Pneumocystis jiroveci cysts using methenamine silver stain (Figure 2). The boy’s prophylaxis dose of TMP-SMX was switched to therapeutic levels, and he improved after 14 days of treatment. He did not require treatment with corticosteroids.

NEXT: Discussion
DISCUSSION
PCP is an opportunistic infection in individuals with decreased cell-mediated immunity, particularly among patients with AIDS and a CD4 count of < 200 cells/mm3.1,2 Nonproductive cough, fever, dyspnea at rest, tachypnea, hypoxia, and increased oxygen requirement are the cardinal features of PCP.1
Our patient had normal oxygen saturation in room air at admission, did not require oxygen support, and had chest radiograph results consistent with community-acquired pneumonia (Figure 1). However, PCP remains high in the differential of patients with low CD4 count and increased LDH who are not taking combination antiretroviral therapy or adhering to PCP prophylaxis.3,4
Classic chest radiograph findings in PCP consist of bilateral diffuse interstitial lung disease; however, PCP may present with unremarkable chest radiograph to cavitary, lobar, miliary, and nodular lung lesions.1,4 In patients with a high number of PCP organisms, clinicians may consider an alternative, less invasive, and less sensitive procedure such as bronchoscopy. Collection of bronchoalveolar lavage specimen may also be considered.1,4 Several stains, including methenamine silver, may be used to identify the thick-walled cysts of P jiroveci (Figure 2).
TMP-SMX is the agent of choice for both prophylaxis and treatment of PCP.1,2 Although we practice medicine in an era in which highly active antiretroviral therapy is available, we must be aware that certain patients, particularly adolescents, may have significant psychosocial and behavioral issues that make adhering to antiretroviral therapy and opportunistic infection prophylaxis difficult. We should work closely with our challenging patients and offer multidisciplinary support, which includes mental health providers, to overcome these issues and improve adherence.
Roberto P. Santos, MD, is a Pediatric Infectious Diseases Attending at Albany Medical Center in New York.
Mary Ellen Adams, RN, is an HIV Coordinator at the Specialized Care Center for Adolescents & Young Adults at Albany Medical Center in New York.
Martha L. Lepow, MD, is a Pediatric Infectious Diseases Attending at Albany Medical Center in New York.
REFERENCES
- American Academy of Pediatrics. Pneumocystis jirovecii Infections. In: Kimberlin DW, Brady MT, Jackson MA, Long SS, eds. Red Book: Report of the Committee on Infectious Diseases. 30th ed. Elk Grove Village, IL: American Academy of Pediatrics; 2015:638-644.
- Panel on Opportunistic Infections in HIV-Infected Adults and Adolescents. Guidelines for the prevention and treatment of opportunistic infections in HIV-infected adults and adolescents: recommendations from the Centers for Disease Control and Prevention, the National Institutes of Health, and the HIV Medicine Association of the Infectious Diseases Society of America. http://aidsinfo.nih.gov/contentfiles/lvguidelines/adult_oi.pdf. Accessed June 21, 2016. B1-B18.
- Wilkin A, Feinberg J. Pneumocystis carinii Pneumonia. Am Fam Physician. 1999;60(6):1699-1708.
- Dixit R, Dixit K. Pneumocystis carinii Pneumonia: an unusual presentation. Indian J Allergy Asthma Immunol. 2003;17(1):29-32.