
An Optimal Treatment Plan to Prevent Lower Extremity Amputations in Patients with Type 2 Diabetes
ABSTRACT: To prevent lower extremity amputation and promote healing in all patients with diabetes, primary care physicians must understand the risk factors and pathophysiology contributing to ulcer formation, obtain a thorough history and physical examination, recognize the complications of ulcers that lead to amputation, and establish optimal treatment plans directed to each patient’s respective needs.
Roughly 8% of Americans suffer from diabetes and 25% to 40% of those people are undiagnosed.1 Because of its many microvascular and macrovascular complications, diabetes management is expensive. Almost 14% of healthcare expenditures in the United States come from diabetes and more than 50% of that is due to complications, such as myocardial infarction, end-stage renal disease, stroke, retinopathy, and foot ulcers.2 A 2014 analysis found that annual healthcare costs ranged from $11,710 to $16,883 per patient with a foot ulcer.3
Diabetes mellitus (DM) is the most common cause of neuropathic foot ulcers in the United States; approximately 25% of the 16 million Americans with diabetes develop a foot ulcer in their lifetime.4 DM causes 85% of all non-traumatic lower extremity amputations in the country, demonstrating the importance of prevention and management of diabetic foot lesions and ulcers.5
To prevent lower extremity amputation and promote healing in all patients with diabetes, especially noncompliant patients, primary care physicians must understand the risk factors and pathophysiology contributing to ulcer formation, obtain a thorough history and physical examination, recognize the complications of ulcers that lead to amputation, and establish optimal treatment plans directed to each patient’s respective needs. This article focuses on efforts provided by doctors in clinical settings.
Pathophysiology and Risk Factors
Diabetic foot ulcers develop secondary to neuropathy, foot deformity, vascular disease, and previous foot ulceration. With sensory neuropathy, the patient experiences decreased protective sensations, thus limiting the sensation of pain and temperature. Autonomic neuropathy causes anhidrosis of the foot—leading to dry, brittle skin and, eventually, fissures, and calluses.6 With decreased autonomic tone in the capillaries, arteries shunt blood directly from arteries into veins resulting in a warm foot with distended veins and bounding pulses.7 Unfortunately, with this malformation, tissues are not properly nourished and the foot is left susceptible to localized gangrene and poor healing.7
Researchers from the European Diabetes Centers Study of Complications in Patients with Insulin-Dependent Diabetes Mellitus study determined that duration of diabetes, glycosylated hemoglobin (HbA1c) levels, triglyceride levels, body mass index (BMI), smoking, and baseline hypertension are associated with the severity of neuropathy.8 Independent of additional risk factors, cardiovascular disease at baseline doubles the risk of neuropathy.7 Neuropathy can lead to feet deformities. Extrinsic muscles eventually overpower atrophied intrinsic muscles, which leads to bony prominences that can ulcerate.2 With repetitive trauma from increased pressure and frictional forces on the bony prominences, ulcers are prone to develop.2
Peripheral artery disease (PAD) is another important risk factor in diabetic foot ulcer development as it impedes wound healing. Diabetes causes increased capillary permeability secondary to thickening of capillary basement membranes, endothelial gap formation, and arteriolar shunting.2,9 Platelet aggregation and increased free radicals lead to capillary damage and oxidative stress. The free radicals reduce nitrous oxide, thus impeding the ability to vasodilate. This becomes especially problematic with neuropathy as the responses to painful stimuli, such as vasodilation, are lost and the standard healing responses to stimuli are compromised.9 PAD disrupts the integrity of the skin and allows minor breaks to grow and possibly become ulcers.6
These risk factors, along with previous ulcer formation, provide clinicians with a way to predict foot ulcer risk in patients with diabetes. The International Working Group on the Diabetic Foot categorized patients as follows10:
• Group 0: No evidence of neuropathy
• Group 1: Neuropathy present without evidence of PAD or foot deformity
• Group 2: Neuropathy with evidence of PAD or deformity
• Group 3: History of foot ulceration or lower extremity amputation
A prospective, case-control study was performed on 225 patients using this classification system to determine the risk of future ulcer formation.11 In the 30 months of follow-up, 5% of patients in group 0, 14% in group 1, 13% in group 2, and 65% in group 3 developed ulcers.11 Only 2% of patients in group 2 and 26% of patients in group 3 eventually had lower extremity amputations.11
History and Physical Examination
A thorough history and physical examination can help physicians assess a patient’s risk for and severity of diabetic foot ulcers. During the history, physicians should learn of the duration of diabetes, glycemic control, history of previous foot ulcers or amputation, history of cigarette smoking, and presence of claudication.12 Peripheral neuropathy, PAD, and duration of diabetes increases the risk of developing foot ulcers.11 If patients describe lower extremity discomfort, clinicians can ask questions to quantify the severity of the symptoms12:
• What is the sensation felt? Score (maximum of 2 points): numbness, burning, or tingling (2 points); aching, cramping, or fatigue (1 point).
• Where are the symptoms? Score (maximum of 2 points): feet (2 points); calves (1 point); anywhere else (0 points).
• Have the symptoms ever awoken you at night? Yes (1 point).
• When do you feel these symptoms? Score (maximum of 2 points): worse at night (2 points); present day and night (1 point); present only during the daytime (0 points).
• How are the symptoms relieved? Score (maximum of 2 points): walking around (2 points); standing (1 point); sitting or lying or no relief (0 points).
The total symptom score is determined for these questions to quantify the severity of symptoms12: normal (0 to 2), mild (3 to 4), moderate (5 to 6), and severe (7 to 9).
Every diabetic patient should have documented foot exams. The examination should focus on peripheral neuropathy, PAD, foot deformities, and the presence of existing ulcers.11 Previous reports have shown that thorough physical examinations are not always performed. One survey of 1434 clinicians in the United States found that only 50% performed semiannual neurologic and foot examinations, per the American Diabetes Association (ADA) recommendations for routine care.13 A second survey of an organization providing care for 14,539 diabetic patients found that 6% of patients had a documented foot examination in the previous year.14
More than 80% of diabetic patients with foot ulcers experience neuropathy.7 The ADA recommends that all patients with type 2 diabetes be screened for neuropathy at diagnosis and at least annually afterwards.15 As patients lose their sensation of pain and perception of balance, they are vulnerable to muscle imbalance, anatomic deformities, and, eventually, foot ulcers.7
Neuropathy is assessed in detail using vibration sensation, pressure sensation, and/or superficial pain or temperature. Clinicians can easily assess vibration sensation using a 128-Hz tuning fork at the bony prominence on the dorsum of the first toe.7 Patients recount both the start and end of vibration, with the test performed twice on each great toe.7 A 2011 study on simple screening tests for peripheral neuropathy as a predictor of diabetic foot ulceration reported that the tuning fork had specificity of 90% and sensitivity of 56%.16
Pressure sensation is determined with a Semmes-Weinstein monofilament.2 Normally, patients with intact sensation can feel a 4.17 monofilament, which equates to 1 g of linear pressure.2 Sensation is considered lost when patients cannot feel a 5.07 monofilament (10 g of linear pressure) on the plantar surface of the foot.2 Insensitivity to the monofilament increases the patients’ likelihood of developing an ulcer on the plantar surface or even future lower extremity amputation.7,17
Superficial pain and temperature can easily be tested, but clinicians do not need to assess both.7 Combining multiple tests together has more than 87% sensitivity in diagnosing diabetic peripheral neuropathy.15 Physicians must keep in mind diabetic peripheral neuropathy and consider other causes, such as neurotoxicity, heavy metal poisoning, alcohol abuse, renal disease, and chronic inflammatory demyelinating neuropathy.15
Clinicians have multiple options to evaluate for PAD. Initially, all clinicians should obtain a history of claudication and assess the pedal pulses.15 Skin temperature, hair, and skin color are somewhat helpful, but they are neither sensitive nor specific.7 All patients with symptoms of PAD should have a diagnostic ankle-brachial pressure index (ABI) testing performed.15 The ADA recommends that all patients over 50 years and those under 50 with risk factors (eg, hypertension, hyperlipidemia, smoking, or a ≥10-year history of diabetes) be screened for PAD using an ABI; those with a positive ABI should be referred for further vascular assessment.15
Physicians treating patients with wounds or ulcers need to do a careful examination of the area. A commonly used wound classification uses Wagner grades and is as follows18:
• Grade 0: No ulcer in a high-risk foot
• Grade 1: Superficial ulcer that involves the entire skin thickness but no underlying tissues
• Grade 2: An ulcer that extends to ligaments and muscles
without bone involvement or abscess development
• Grade 3: Deep ulcer with cellulitis or abscess, often includes
osteomyelitis
• Grade 4: Localized gangrene
• Grade 5: Extensive gangrene involving the whole foot
Physicians should examine the ulcer for odor, drainage, granulation tissue, and exposure to underlying anatomy.7 These findings will help to determine the likelihood of an infection.
An infection is considered if a patient has 2 of the following: tenderness, erythema, swelling, warmth, or pus exiting from an ulcer site and/or nearby sinus tract.7 Osteomyelitis should be considered, and is likely present, if a deep ulcer exposes bone or if a bone can be easily probed with a sterile, blunt, stainless steel object.7
Complications
Using the above physical examination findings, physicians can recognize and hopefully limit the complications of diabetic foot ulcers. Diabetic patients are more susceptible to infections and physicians must recognize them early to limit the chances of osteomyelitis and sepsis. Diabetes limits immunological response by reducing polymorphonuclear leukocyte function along with humoral and cell-mediated immunity.19
Three steps are used to evaluate a patient with a diabetic foot infection6:
1. Verify the severity of infection
2. Consider underlying factors predisposing and promoting infection
3. Determine the microbial etiology
The Infectious Disease Society of America recommends that clinicians evaluate patients with diabetic foot infections at 3 levels: the patient as a whole, the affected foot or extremity, and the infectious wound.19 Observing the whole patient, doctors should evaluate for signs of systemic infection, such as fever, chills, diaphoresis, tachycardia, hypotension, and delirium.19 Laboratory findings suggesting systemic infection include leukocytosis, a left-shifted leukocyte differential, elevated C-reactive protein, elevated erythrocyte sedimentation rate (ESR), and elevated procalcitonin.19 Systemic signs should point clinicians to a severe infection with either significant tissue involvement and/or more virulent pathogens.19
Next, physicians should examine the extremity and foot for localized infection spread. Proximal infectious spread is considered with contiguous skin, lymphatic channels, and/or regional lymph node involvement.19 Also, foot deformities limit a patient’s ability to heal from a wound or ulcer. At this point, if an ABI has not been done to assess for PAD, it should be done to determine if decreased vascular supply is limiting wound healing. Physicians can simply evaluate for the presence or absence of pedal pulses if time is limited.19
Finally, after evaluating the patient as a whole and his or her extremity, physicians determine the severity of the infectious wound. First, physicians should debride any necrotic material or callus, and then gently probe the area to determine the presence of abscesses, sinus tracts, foreign bodies, or any bone or joint involvement.19 Patients can expect necrotizing tissue infections in ulcers with soft tissue gas, foul odor, cutaneous bullae, and skin discoloration.20 Next, the wound size and depth should be documented for reference at subsequent examinations. Finally, clinicians should obtain wound cultures for correct antibiotic therapy.19
Diabetic foot infections are often polymicrobial in nature and vary depending on the tissue involvement. Superficial foot infections are most likely due to aerobic gram-positive cocci (eg, Staphylococcus aureus, Streptococcus agalactiae, S pyogenes and coagulase-negative staphylococci).20 Deeper ulcers, those that are more chronically infected, or those previously treated with antibiotics are more likely to be polymicrobial.20 These ulcers involve the previously mentioned bacteria as well as enterococci, Enterobacteriaceae, Pseudomonas aeruginosa, and anaerobes.20 P aeruginosa is common in diabetic foot infections in warm climates. Patients exposing their ulcers to water or moist environments also increase the risk of P aeruginosa infection.20 Finally, more extensive wounds with malodorous drainage, necrosis, or gangrene with possible systemic toxicity are prone to anaerobic infections involving anaerobic streptococci, Bacteroides species, and Clostridium species.20
Osteomyelitis, with or without soft tissue infection, can occur in diabetic foot wounds.20 Osteomyelitis can be difficult to diagnose because signs and symptoms of infection can be absent or limited due to vascular disease and neuropathy.21Clinicians should observe changes in the foot, such as deformities, neuropathy, tenderness, and venous or arterial insufficiency.21
Doctors should also take note to the size of the ulcer as those more than 2 cm2 are more likely to have osteomyelitis than smaller ulcers.21 A probe-to-bone test, as described above, is helpful in determining the presence of osteomyelitis.21 An ESR >70 mm/hour or positive findings on radiographs are helpful in diagnosis.21 Wound temperature, ulcer inflammation, elevated white blood cell count, and swab cultures are not as useful in determining if a patient has osteomyelitis nor does it lead to a therapy plan.21
Treatment
Clinicians have many treatment options available for diabetic foot ulcers and their complications. First and foremost, it is paramount that physicians educate their patients on proper glycemic control with pharmacological assistance and lifestyle adjustments. The ADA recommends HbA1c testing at least twice per year in patients who are meeting glycemic control and quarterly for those not meeting their glycemic goals.15 Lowering HbA1c to <7% can reduce microvascular disease.15 In patients at risk for hypoglycemia, limited life expectancy, extensive comorbid conditions, preexisting microvascular and macrovascular complications, or those with a long history of diabetes with difficult control, physicians should encourage an HbA1c <8%. Evidence suggests that educating patients to self-manage their diabetes improves HbA1c levels, decreases weight, improves quality of life, and lowers costs.15 The best way to treat diabetic foot ulcers is to prevent them from happening.
Hydrocolloid dressings are recommended as they absorb, aid in autolysis, and can be left on for several days.22 However, they also make wounds more malodorous and prone to maceration along with an increased risk for infection.22
In the aforementioned case, our patient used Duoderm dressings for the first few weeks and they seemed to help with smaller ulcers. However, the efficacy was somewhat hindered given that our patient was on his feet at work while using the dressings.
As clinicians observe the continuing development of antibiotic-resistant bacteria, it is imperative to consider all possible options to protect against these pathogens. Honey has been shown to inhibit bacterial growth either due to its antimicrobial properties or to its acidity and hyperosmolar nature.23 Topical honey promotes autolytic debridement and healing by stimulating growth of wound tissues, which decreases edema, pain, and exudate production.23 Given the severity of our patient’s diabetes, medical honey was beneficial but not sufficient to resolve his infection. His wound cultures displayed a multitude of organisms on multiple occasions.
Our patient made significant improvement with negative pressure wound therapy (NPWT). It works using a foam sponge compressed by suction, which induces microdeformations in the wound surface.24 These wound changes lead to cell proliferation and angiogenesis stimulation.24 The mechanical forces from NPWT facilitate wound closure using physical wound contraction and increased cellular response to mechanic stresses. NPWT provides a moist healing environment, increases granulation tissue formation, and removes exudate from the wound bed.24 NPWT offers multiple advantages compared to traditional therapy of moist saline dressings that are changed 3 times daily. NPWT dressings need fewer changes (every 2 to 3 days) compared to traditional therapy and accelerate the rate of wound healing and return to baseline.25, 26
NPWT is more expensive than traditional wound therapy—but costs can vary depending on the frequency of dressing changes. NPWT is considered safe and complications usually only occur when it is applied to wounds with devitalized tissue or exposed vital structues.25 Bleeding is the most serious complication, which is usually associated with granulation tissue at the base of wound. When patients using NPWT present with infections it is often due to an inadequately controlled previous infection prior to NPWT. In these particular cases, physicians should discontinue NPWT, cleanse and debride the wound, obtain cultures, and start empiric antibiotic therapy.25
In determining an antibiotic regimen for infectious diabetic ulcers, clinicians must determine the severity of infection as it plays a key factor in the prognosis and management options. Mild infections include at least 3 of the following: purulence, erythema, pain, tenderness, warmth, or induration. Note: Any cellulitis is <2 cm and involves only the skin or superficial subcutaneous tissues.19 Moderate infections are as described for mild infections, but erythema is >2 cm or involves deeper structures than skin or subcutaneous tissues. Severe infections are classified as a local infection with positive systemic inflammatory response syndrome criteria.19
Clinicians can treat mild infections with outpatient oral antimicrobial therapy.20 These infections typically involve skin flora, such as streptococci and S aureus.20 If patients do not respond to treatment therapy directed against streptococci and methicillin-susceptible S aureus (MSSA), clinicians should provide extended coverage against methicillin-resistant S aureus (MRSA), aerobic gram-negative bacilli, and anaerobes.20 Risk factors for MRSA include previous MRSA infection, prior antibiotic use, previous hospitalization, and residence in long-term care facility.20 In our case, we elected to treat the patient’s initial infection with cephalexin.
Moderate infections that involve the fascia should have antimicrobial coverage against streptococci, MSSA, and MRSA if risk factors are present, anaerobes, and aerobic gram-negative bacilli.20 Physicians dealing with extensive infections involving deep tissues should arrange for patients to receive empiric parenteral therapy.20
Severe, limb-threatening infections, and those with systemic infections, should receive broad-spectrum parenteral antibiotic therapy.20 Our patient responded well to parenteral coverage with meropenum and ampicillin-sulbactam. In cases of osteomyelitis, clinicians should provide parenteral treatment similar to that for moderate or severe infections. Clinicians should obtain cultures and direct antimicrobial treatment accordingly.20
In our case study, the patient developed significant debilitating ulcers and cellulitis that threatened his limb. However, through proper education on proper glycemic control and with multiple treatment options tailored to his specific needs, he has made significant progress. As clinicians, we must understand the pathophysiology of diabetic foot conditions and proper physical examination techniques to limit complications of diabetic foot and provide thorough and effective treatment that improves quality of life and limits potential lower extremity amputations.
A Case Study
A 42-year-old male with type 2 diabetes complained of a non-healing, enlarging, and swollen wound on the left medial plantar surface over the first metatarsal.
History
In the year prior, he had a cervical spine fusion, which he said significantly limited the function of his right leg and made him constantly place his body weight on the left leg. He developed neuropathy secondary to the diabetes and eventually formed an ulcer. The lesion was debrided revealing Wagner grade 2 ulcer (Figure 1).
Physical Examination
The patient had a BMI of 41.6, HbA1c of 11.2%, and home blood glucose levels >300.

Initial Treatment and Follow-Up
We applied a Duoderm patch, instructed him on how to change the dressing, and requested a biweekly follow-up.
As he continued to work over the next month and put stress on his left foot, he developed a second ulcer (Figure 2) on the lateral plantar surface over the left fifth metatarsal. He related that with his neuropathy he felt little tenderness leading to its rapid growth. With regular debridement and dressing changes, we were able to stop the growth of both ulcers.
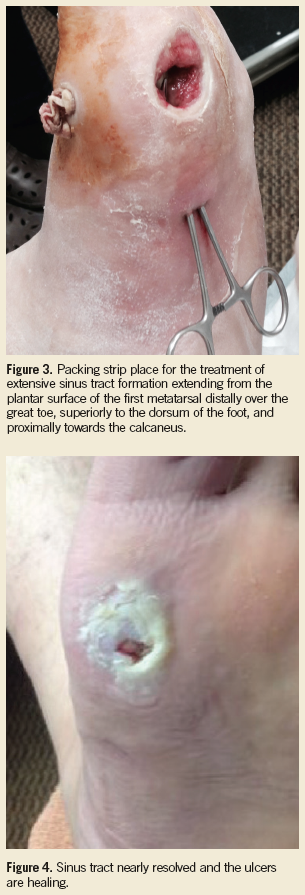
Over the following weeks, he continued to bear weight on his foot, a requirement for work, and developed a sinus tract from a third ulcer located over the first metatarsal extending distally to his great toe and proximally on the medial aspect of his plantar surface. We obtained wound cultures, packed the tract with iodoform packing strips (Figure 3), and started oral antibiotic therapy.
Laboratory Tests
The culture showed 3+ Escherichia coli, 2+ Enterococcus faecalis, 2+ Candida albicans, 2+ Bacteroides fragilis, 2+ anaerobic gram-negative Bacillus and 1+ Peptostreptococcus anaerobius. He showed minimal response to oral antibiotic coverage and the concern for potential limb loss grew.
Treatment
Based upon the results of the culture and sensitivity, we determined that an aggressive antibiotic treatment was needed. A peripherally inserted central catheter was placed for mero-penem and ampicillin-sulbactam delivery for 1 week. As his infection improved over the next few weeks, we continued with regular wound debridement and bandage placement and encouraged him to use the walking boot provided for him. The patient also went on disability, which decreased the amount of time he was standing. We also tried an array of topical treatments such as hydrogel, medical honey, bacitracin ointment, and lidocaine cream.
While these treatment options prevented infection and slowly decreased the ulcer size, we elected to advance our treatment to negative pressure wound therapy (NPWT). We changed the NPWT biweekly and the ulcer decreased dramatically in size (Figure 4).
Outcome of the Case
With pressure relief from a walking boot, regular debridement, topical therapy, NPWT, and lowered HbA1c to 9.2%, this patient is close to being ulcer free.
This article was originally published in the May issue of The Dermatologist.
References:
- American Diabetes Association. Standards of medical care in diabetes—2010. Diabetes Care. 2010;33(suppl 1):S11-S61.
- Lin P, Phillips T. Ulcers. In: Blognia J, Jorrizo, J, Rapini R. Dermatology. Vol 2. Philadelphia, PA: Elsevier; 2003:1631-1649.
- Rice JB, Desai U, Cummings AK, et al. Burden of diabetic foot ulcers for medicare and private insurers. Diabetes Care. 2013;37(3):651-658.
- Boulton AJ, Kirsner RS, Vileikyte L. Clinical practice. Neuropathic diabetic foot ulcers. N Engl J Med. 2004;351(1):48-55.
- Boulton AJ, Armstrong DG, Albert SF, et al. Comprehensive foot examination and risk assessment: a report of the task force of the foot care Interest Group of the American Diabetes Association, with endorsement by the American Association of Clinical Endocrinologists. Diabetes Care. 2008;31(8):1679-1685.
- Powers A. Diabetes mellitus. In: Longo DL, Fauci AS, Kasper DL, et al. eds. Harrison’s Principles of Internal Medicine. 18th ed. New York, NY: McGraw-Hill; 2012:chap 44.
- McCulloch D. Evaluation of the diabetic foot. UpToDate. www.uptodate.com/contents/evaluation-of-the-diabetic-foot.
- Accessed April 17, 2015.
- Tesfaye S, Chaturvedi N, Eaton SE, et al. Vascular risk factors and diabetic neuropathy. N Engl J Med. 2005;352(4):341-350.
- Forsythe RO, Brownrigg J, Hinchliffe RJ. Peripheral arterial disease and revascularization of the diabetic foot. Diabetes Obes Metab. 2015;17(5):435-444.
- Apelqvist J, Bakker K, van Houtum WH, et al.
- International consensus and practical guidelines on the management and the prevention of the diabetic foot. International Working Group on the Diabetic Foot. Diabetes Metab Res Rev. 2000;16(suppl 1):S84-S92.
- Peters EJ, Lavery LA. Effectiveness of the diabetic foot risk classification system of the International Working Group on the Diabetic Foot. Diabetes Care. 2001;24(8):1442-1447.
- Young MJ, Boulton AJ, MacLeod AF, et al. A multicentre study of the prevalence of diabetic peripheral neuropathy in the United Kingdom hospital clinic population. Diabetologia. 1993;36(2):150-154.
- Kenny SJ, Smith PJ, Goldschmid MG, et al. Survey of physician practice behaviors related to diabetes mellitus in the U.S. Physician adherence to consensus recommendations. Diabetes Care. 1993;16(11):1507-1510.
- Peters AL, Legorreta AP, Ossorio RC, Davidson MB. Quality of outpatient care provided to diabetic patients. A health maintenance organization experience. Diabetes Care. 1996;19(6):601-606.
- American Diabetes Association. Standards of medical care in diabetes—2013. Diabetes Care. 2013;36(suppl 1):S11-S66.
- Perkins BA, Olaleye D, Zinman B, Bril V. Simple screening tests for peripheral neuropathy in the diabetes clinic. Diabetes Care. 2001;24(2):250-256.
- Morshed GM, Mashahit MA, Shaheen HA. Simple screening tests for peripheral neuropathy as prediction of diabetic foot ulceration. FAOJ. 2011;4(11):2.
- Mayfield JA, Sugarman JR. The use of the Semmes-Weinstein monofilament and other threshold tests for preventing foot ulceration and amputation in persons with diabetes. J Fam Pract. 2000;49(11 suppl):S17-S29.
- O’Neal LW, Wagner FW. The Diabetic Foot. St Louis, MO: Mosby; 1983:274.
- Lipsky BA, Berendt AR, Cornia PB, et al. 2012 Infectious Diseases Society of America clinical practice guideline for the diagnosis and treatment of diabetic foot infections. Clin Infect Dis. 2012;54(12):e132-e173.
- Weintrob A, Sexton D. Clinical manifestations, diagnosis, and management of diabetic infections of the lower extremities. UpToDate. www.uptodate.com/contents/clinical-manifestations-diagnosis-and-management-of-diabetic-infections-of-the-lower-extremities. Accessed April 17, 2015.
- Butalia S, Palda VA, Sargeant RJ, et al. Does this patient with diabetes have osteomyelitis of the lower extremity? JAMA. 2008;299(7):806-813.
- Hilton JR, Williams DT, Beuker B, et al. Wound dressings in diabetic foot disease. Clin Infect Dis. 2004;39(suppl 2):S100-S103.
- Al-Waili N, Salom K, Al-Ghamdi AA. Honey for wound healing, ulcers, and burns; data supporting its use in clinical practice. ScientificWorldJournal. 2011;11:766-787.
- Capobianco CM, Zgonis T. An overview of negative pressure wound therapy for the lower extremity. Clin Podiatr Med Surg. 2009;26(4):619-631.
- Gestring M. Negative pressure wound therapy. UpToDate. www.uptodate.com/contents/negative-pressure-wound-therapy. Accessed April 17, 2015.
- Blume PA, Walters J, Payne W, et al. Comparison of negative pressure wound therapy using vacuum-assisted closure with advanced moist wound therapy in the treatment of diabetic foot ulcers: a multicenter randomized controlled trial. Diabetes Care. 2008;31(4):631-636.