
Interactive Quiz: Pruritic Rash Involving the Eyebrows
Welcome to Consultant360's latest interactive diagnostic quiz. Over the next few pages, we'll present a case and ask you to make the diagnosis and treat the patient. Along the way, we'll provide details about the case, and at the end, we'll share the patient's outcome.
First, let's meet the patient.
A 69-year-old woman presented with a pruritic rash involving her eyebrows, associated with lymphadenopathy of her face and neck. The lesions had developed within a week of her having had her eyebrows tattooed while in Thailand. She stated that the lesions had ruptured, had drained purulent bloody discharge, and then had crusted. Upon returning to the United States, she had been evaluated in an urgent care clinic, where she had been prescribed a regimen of clindamycin for a presumed diagnosis of cellulitis.
Although the lesions initially had improved with clindamycin, after a few days, the pruritic, papulonodular lesions over her eyebrows had returned. After the rash had failed to improve with a second course of clindamycin, she had been referred to an infectious disease clinic.
At presentation, physical examination findings were notable for the presence of erythematous nodules overlying the tattooed area (Figure 1), with associated scaling and dryness, along with tender, freely mobile preauricular and anterior cervical lymphadenopathy (Figure 2). The rest of the physical examination findings were unremarkable.


The physicians diagnosed this condition as cutaneous Mycobacterium haemophilum infection.
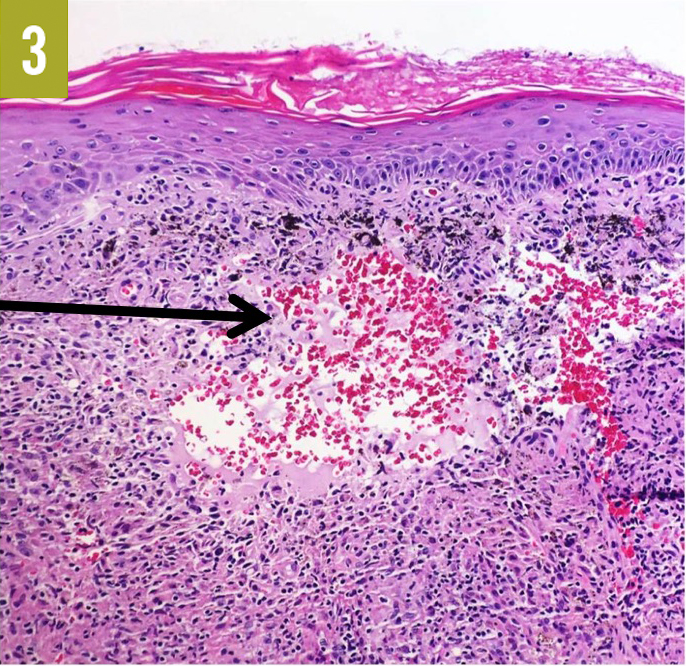
The patient was referred to a dermatologist for a punch biopsy of the eyebrow lesion, and the specimen was sent for histopathology and culture studies. Routine hematoxylin-eosin staining showed multiple necrotizing granulomas occupying the dermis (Figure 3), and acid-fast bacilli (AFB) and Fite special staining highlighted a few scattered mycobacterial organisms (Figure 4). Fungal staining results were negative. AFB, fungal, and bacterial cultures were negative at 6 weeks. An additional biopsy was performed, this time of the lymph nodes, and the specimen was sent for culture studies. The AFB cultures were incubated at a lower temperature of 28°C, which eventually allowed for growth of the organism.

Answer: B. Polymerase chain reaction assay
Growth on the mycobacterial culture media was noted at approximately 4 weeks of incubation. The specimen was then sent for 16S rRNA polymerase chain reaction assay and was identified as Mycobacterium haemophilum. Mycobacterial susceptibility testing with agar disk elution, performed at an outside laboratory, revealed the organism to be resistant to amikacin but susceptible to clarithromycin, rifampin, trimethoprim-sulfamethoxazole, linezolid, ciprofloxacin, doxycycline, and minocycline.
The patient was treated with triple therapy with ciprofloxacin, clarithromycin, and rifampin.
After review of the resistance profile and of other regimens used to treat M haemophilum infection, the patient was started on a regimen of 500 mg of ciprofloxacin twice daily, 500 mg of clarithromycin daily, and 600 mg of rifampin daily, which she tolerated without adverse effects. After 2 months of therapy, her eyebrow lesions had resolved, although the lymphadenopathy had not completely resolved (Figures).


References
Authors:
Heather S. Pomerantz, MD, is a physician in the Department of Infectious Disease at San Antonio Military Medical Center in San Antonio, Texas.
David Chang, MD, is a physician in the Department of Infectious Disease at San Antonio Military Medical Center in San Antonio, Texas.
Margaret J. Abuzeid, MD, is a physician in the Department of Pathology at San Antonio Military Medical Center in San Antonio, Texas.
Brian K. White, DO, is a physician in the Department of Infectious Disease at San Antonio Military Medical Center in San Antonio, Texas.
References:
- Islam PS, Chang C, Selmi C, et al. Medical complications of tattoos: a comprehensive review. Clin Rev Allergy Immunol. 2016;50(2):273-286.
- Kazandjieva J, Tsankov N. Tattoos: dermatological complications. Clin Dermatol.2007;25(4):375-382.
- Frew JW, Nguyen RTD. Tattoo-associated mycobacterial infections: an emerging public health issue. Med J Aust. 2015;203(5):223.
- Drage LA, Ecker PM, Orenstein R, Phillips PK, Edson RS. An outbreak of Mycobacterium chelonae infections in tattoos. J Am Acad Dermatol. 2010;62(3):501-506.
- Centers for Disease Control and Prevention (CDC). Tattoo-associated nontuberculous mycobacterial skin infections—multiple states, 2011-2012. MMWR Morb Mortal Wkly Rep.2012;61(33):653-656.
- Falsey RR, Kinzer MH, Hurst S, et al. Cutaneous inoculation of nontuberculous mycobacteria during professional tattooing: a case series and epidemiologic study. Clin Infect Dis. 2013;57(6):e143-e147.
- Philips RC, Hunter-Ellul LA, Martin JE, Wilkerson MG. Mycobacterium fortuitum infection arising in a new tattoo. Dermatol Online J. 2014;20(6). https://escholarship.org/uc/item/6bs3q0h0. Published January 1, 2014. Accessed February 7, 2018.
- Kay MK, Perti TR, Duchin JS. Tattoo-associated Mycobacterium haemophilum skin infection in immunocompetent adult, 2009. Emerg Infect Dis. 2011;17(9):1734-1736.
- Giulieri S, Morisod B, Edney T, et al. Outbreak of Mycobacterium haemophilum infections after permanent makeup of the eyebrows. Clin Infect Dis. 2011;52(4):488-491.
- Saubolle MA, Kiehn TE, White MH, Rudinsky MF, Armstrong D. Mycobacterium haemophilum: microbiology and expanding clinical and geographic spectra of disease in humans. Clin Microbiol Rev. 1996;9(4):435-447.
- Shah MK, Sebti A, Kiehn TE, Massarella SA, Sepkowitz KA. Mycobacterium haemophilum in immunocompromised patients. Clin Infect Dis. 2001;33(3):330-337.
- Griffith DE, Aksamit T, Brown-Elliott BA, et al; ATS Mycobacterial Diseases Subcommittee. An official ATS/IDSA statement: diagnosis, treatment, and prevention of nontuberculous mycobacterial diseases. Am J Respir Crit Care Med. 2007;175(4):367-416.
- Pfyffer GE. Mycobacterium: general characteristics, laboratory detection, and staining procedures. In: Jorgensen JH, Pfaller MA, Carroll KC, et al, eds. Manual of Clinical Microbiology. Vol 1. 11th ed. Washington, DC: ASM Press; 2015:chap 30.
- Gonzalez-Santiago TM, Drage LA. Nontuberculous mycobacteria: skin and soft tissue infections. Dermatol Clin. 2015;33(3):563-577.
Disclaimer:
The views expressed in this article are those of the authors and do not reflect the official policy or position of the Uniformed Services University of the Health Sciences; the Departments of the Army, Navy, or Air Force; the Department of Defense; or the US Government.