
Improving Patient Care with Intensive Visiting Faculty Workshops: A Practice-Based Case Study
As the clinicians most often involved in the care of patients with type 2 diabetes, the ability of primary care providers to overcome clinical inertia and patient- and provider--
related barriers to aggressive therapy escalation—including the early initiation of insulin—is paramount to achieving glycemic control and preventing diabetes-related microvascular and macrovascular complications in this patient population.1,2 Yet, misconceptions regarding insulin, the high percentage of patients with type 2 diabetes who are not achieving ADA glycemic goals, and the significant morbidity and mortality associated with this progressive disease suggest that room for improvement exists in the care of patients with type 2 diabetes.3,4 The Transforming Your Primary Care Group Practice into a Center of Excellence in Type 2 Diabetes Care workshop series seeks to provide high-intensity, hands-on education for the multidisciplinary healthcare team, designed to advance primary care practices in areas with a high prevalence of type 2 diabetes (ie, the “Diabetes Belt”) into centers of excellence in type 2 diabetes management.
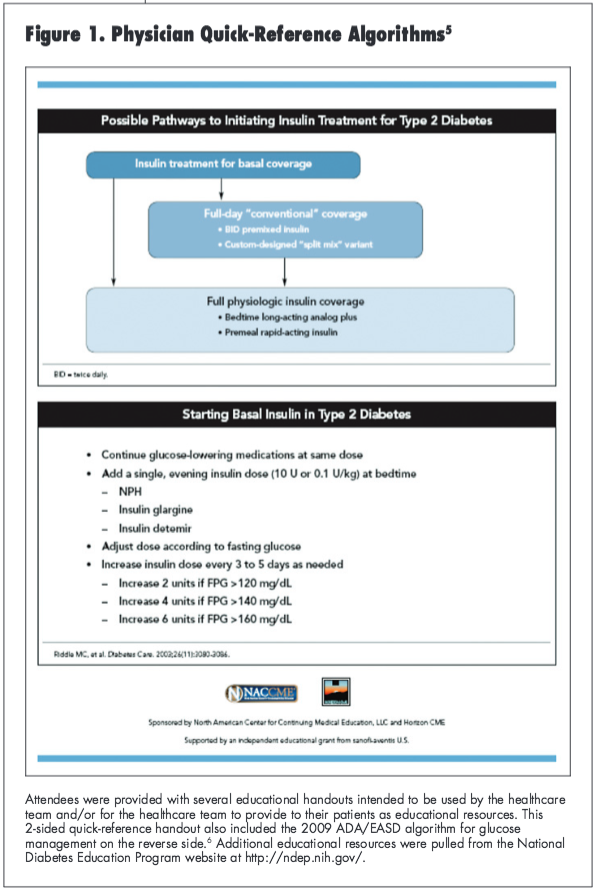
Each intensive workshop was led by a member of the faculty panel, which comprised 7 experts in type 2 diabetes management. Participating practices were asked to select a faculty member of their choice to come to their office and were encouraged to prepare their own patient cases so that the discussion could be tailored to the specific needs of that practice. Through a combination of didactic lecture, interactive question and answer, and case-based discussion, the visiting faculty explored with participants the rationale for early and aggressive glucose management and offered guidance on how to improve patient care within their practice. Participants were provided with a variety of checklists, quick-reference algorithms, and patient education materials to foster guideline-directed care, meaningful communication with patients, and patient engagement in optimizing type 2 diabetes care (Figure 1).5 The goal of each workshop was to empower the healthcare team to appropriately and successfully treat every patient with type 2 diabetes within their practice.
In addition to the educational materials provided to participants, attendees were also asked to complete a brief pretest at the beginning of the workshop, a program evaluation at the conclusion of the activity, and then a follow-up survey 30 to 45 days post-program. Pre- and immediate post-activity outcomes surveys were used to objectively measure baseline declarative and procedural knowledge and confidence, as well as immediate changes; the follow-up survey will serve to objectively gauge knowledge and confidence retention and measure self-reported performance change. Participants were also asked to complete a long-term chart audit in which they would follow patients over their next 4 clinic visits (or up to 1 year), the results of which will measure the impact of the visiting faculty workshops on clinical decision—making and patient health with specific measures of change including time to escalation of therapy, therapies prescribed during escalation, and percentage change in both HbA1c and patients achieving HbA1c goals. The preliminary findings from these evaluation tools have offered valuable insight into the nature of diabetes care in the primary care setting, both through anecdotal evidence relayed by participants, as well as from the collected survey data.
Practice-Specific Findings
The first visiting faculty workshop of this series occurred at a federally qualified, nonprofit primary care group practice located in an urban area of Florida. This practice employs approximately 30 primary care providers (ie, 20 physicians and 10 nurse practitioners), in addition to staff nurses and medical assistants. Fourteen practice employees attended the workshop (6 physicians, 1 nurse practitioner, and 7 nurses/medical assistants). On average, each of these practitioners sees 39 patients with type 2 diabetes per month, with more than half of the attendees reporting that they treat 50 or more patients with this condition monthly.
The group’s medical director requested a workshop in response to common challenges she noticed in caring for this patient population. For example, due to limited resources, the practice cannot afford to hire a certified diabetes educator and instead relied heavily on the physicians and/or nurse practitioners to provide diabetes education during office visits. To maintain their patient load, however, visits are restricted to 15 minutes, greatly limiting the amount of time available for educating patients about their disease. The medical director also had concerns regarding clinical inertia and thought a new perspective on diabetes management from a visiting faculty would be beneficial for the practice. In asking the practice what they hoped to gain from the workshop, Dr. Rosemarie Lajara—the faculty mentor for this program—noted that many of the participants echoed the sentiments of the medical director in expressing apprehension toward initiating more aggressive therapy, including the use of insulin, with some even wondering if patients requiring insulin should be solely managed by an endocrinologist. They also talked openly about the limited resources and pressures they felt to treat a large number of patients in a short amount of time.
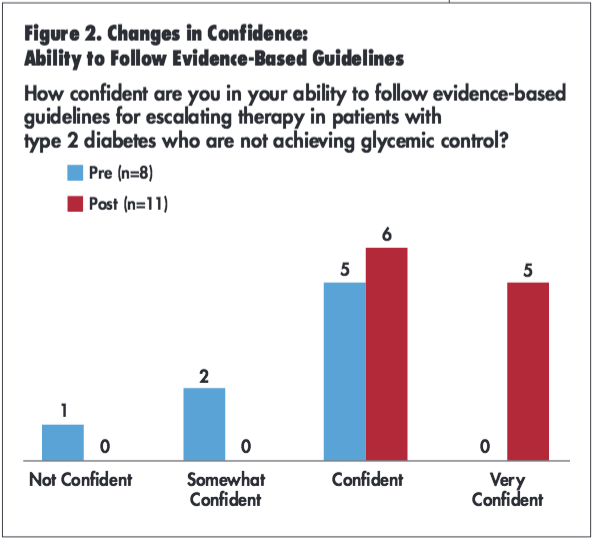
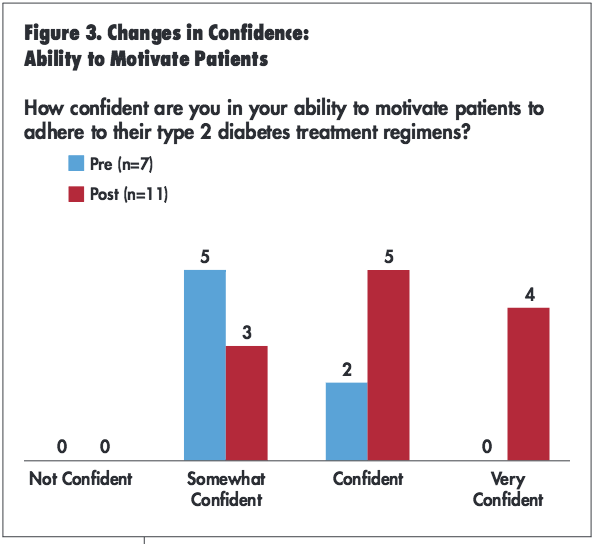
One of the most impressive findings from the group’s pre- and immediate post-activity surveys was the immediate shift in confidence regarding evidence-based guideline recommendations. Participants were asked, how confident are you in your ability to follow evidence-based guidelines for escalating therapy in patients with type 2 diabetes who are not achieving glycemic control? Before participating in the workshop, approximately 60% of respondents were confident in their ability to follow evidence-based guidelines for escalating therapy, while none reported being very confident. Immediately following the activity, all attendees reported being either very confident or confident (Figure 2). Similarly, the percentage of participants who described themselves as very confident or confident in their ability to motivate patients to adhere to their type 2 diabetes treatment regimens prior to the visiting faculty workshop increased from 28.5% to 75% based on pre- and immediate post-activity surveys, respectively (Figure 3). In reviewing these findings, Dr. Lajara was excited to see that the education she provided, in combination with some of the practical advice suggested during the workshop, had a substantial impact on the practice. A key “take-home point” emphasized by Dr. Lajara over the 2-day program was the importance of following treatment protocols (eg, evidence-based algorithms) that establish certain parameters for the intensification of treatment, both as a means of providing consistent and efficient care and also for building confidence in selecting the correct treatment for each patient. An appreciation for the evidence-based guideline recommendations and adherence to therapy may assist clinicians in overcoming clinical inertia through the early escalation of therapy with basal insulin for those who are not well controlled on metformin and lifestyle modifications alone.5
In addition to improvements in confidence, interim findings suggest that the workshop series has the potential to greatly impact patient care via tangible practice modifications. In fact, all participants who completed the post-activity survey indicated that they intended to make a change to their practice based on the program’s teachings (n=12). In speaking with this clinic’s medical director approximately 3 months after the workshop, she stated that her team has initiated insulin in several patients for whom they had previously been reluctant to escalate therapy. Rather than prescribe additional oral agents, they decided to start insulin therapy in an attempt to aggressively gain control of glycemic levels in certain patients and have had good results. In reviewing these practice changes, the medical director also confirmed that the practice had started using the patient and provider education materials to improve patient care. These handouts have been used to train non-physician employees on ways to better educate patients on taking control of their type 2 diabetes, thereby allowing the physicians to focus on more clinical aspects of patient care including initiation of new therapies, medication titration, etc. This change was very much in line with another of Dr. Lajara’s key messages that patients with diabetes require a team effort for proper disease management so that no one member of the team is overwhelmed with the burden of treating this chronic disease. In summary, the medical director found this collaborative effort to be a worthwhile experience that brought together the entire healthcare team to improve patient care.
Conclusion
With overwhelming evidence to support the aggressive pursuit of glycemic goals, including the appropriate use of insulin therapy,6 it is clear that the patients in these clinics will benefit from their practitioners’ participation in this workshop series. And for those who are not able to host a live event, it is our hope that readers of this supplement are able to implement key recommendations into their own practices to provide excellent diabetes care.
References
1. National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK). National diabetes statistics, 2011. http://diabetes.niddk.nih.gov/dm/pubs/statistics/#Kidney. Accessed February 21, 2012.
2. Stratton IM, Adler AI, Neil HA, et al. Association of glycaemia with macrovascular and microvascular complications of type 2 diabetes (UKPDS 35): prospective observational study. BMJ. 2000;321(7258):405-412.
3. Del Prato S, Felton AM, Munro N, et al. Improving glucose management: ten steps to get more patients with type 2 diabetes to glycaemic goal. Int J Clin Pract. 2005;59(11):1345-1355.
4. Brown JB, Nichols GA, Perry A. The burden of treatment failure in type 2 diabetes. Diabetes Care. 2004;27(7):1535-1540.
5. Riddle MC, Rosenstock J, Gerich J; Insulin Glargine 4002 Study Investigators. The treat-to-target trial: randomized addition of glargine or human NPH insulin to oral therapy of type 2 diabetic patients. Diabetes Care. 2003;26(11):3080-3086.
6. Nathan DM, Buse JB, Davidson MB, et al. Medical management of hyper-glycemia in type 2 diabetes: a consensus algorithm for the initiation and adjustment of therapy: a consensus statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care. 2009;32(1):193-203.