
How Would You Diagnose This Patient’s Lesion with Mass Effect?
A 28-year-old white male with past medical history of poorly-controlled Crohn’s disease and drug abuse was admitted to the family medicine inpatient service for abdominal pain and hematochezia of a 2-week duration.
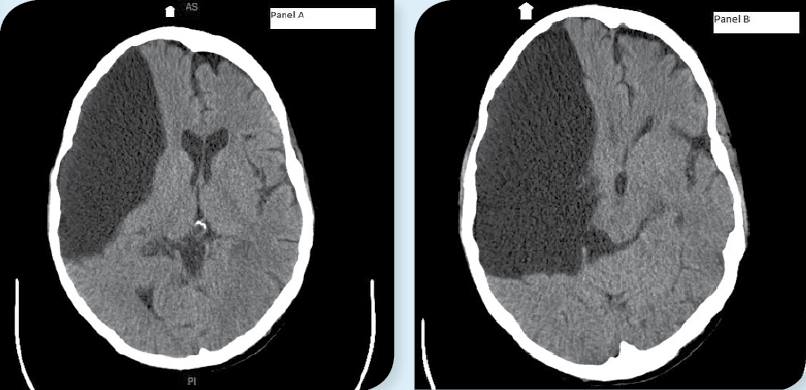
Over the next 5 days, while being treated for a Crohn’s exacerbation with superimposed Clostridium difficile infection, the patient’s hemoglobin levels trended from 12.1 g/dL to 6.6 g/dL. Transfusion orders were placed. While awaiting blood products, the patient had a syncopal episode in the bathroom and hit his head, breaking the drywall. The patient was transferred to the critical care unit, where a CT without contrast of the head and neck revealed what initially appeared to be a large subdural hematoma with midline shift (Figure).
The patient had no neurological deficits. Upon questioning, he reported that he has had a brain cyst since birth that he forgot to mention before the CT.
Upon further evaluation, the fluid in the lesion was a lighter density than blood and it appeared to communicate with the subarachnoid space.
What's your diagnosis?Answer: Porencephalic Cyst
The final read of the CT reported a very large porencephalic cyst in the right hemisphere and right middle cranial fossa with associated atrophy and dysplasia of the right parietal lobe with moderate mass effect, resulting in a 2 cm subfalcine shift to the left.
This cyst had been slowly growing for several years, which could explain the lack of side effects from a lesion this size. He under the care of a neurologist at a neighboring hospital with periodic imaging until such time that the mass became symptomatic and the risk of continued monitoring outweighed the risk of surgical intervention. Endoscopic drainage would be the most likely approach if this were required.1
Discussion
Congenital porencephalic cysts—cerebrospinal fluid-filled brain cysts that lined with white matter—are extremely rare.2,5 They are created in utero or shortly after birth and can be found in any lobe of the brain.2,4 Porencephalic cysts are connected to the ventricular system (Figure 2). Their cause is unknown, but thought to be due to fetal stroke or infection—leading to liquefactive necrosis, which creates a pocket for fluid.2 Prognosis is widely variable depending on the size and location of the cyst, however sequelae of porencephaly can include epilepsy, macrocephaly or microcephaly, spasticity or hypotonia, limited speech, and cognitive impairment.5
Porencephalic cysts are differentiated from neuroglial, arachnoid, and schizencephalic cysts in several ways. Neuroglial cysts, for example, do not communicate with the ventricles as porencephalic cysts do.4 Arachnoid cysts do not originate in the brain, and are therefore considered extra-axial.4 Finally, schizencephalic cysts are lined with grey matter and not white matter.4
Differential Diagnosis
The differential diagnosis for a lesion with mass effect seen on CT includes cyst, abscess, hemorrhage/hematoma, and tumor/metastasis.3 Based on the patient’s circumstances, we initially misinterpreted the patient’s head CT as a large subdural bleed, although an abscess could have also been considered based on the patient’s history of drug abuse. This is an example of a cognitive error (misinterpreting data) as opposed to a perceptual error (not recognizing a finding). We reevaluated the images based on the patient’s lack of neurological deficits as well as our conversation with the patient about his past medical history leading to the correct diagnosis.
Outcome of the Case
The patient in this scenario had no debilitating side effects from his cyst, although it was postulated whether his risky social behaviors could be partly attributed to frontal lobe damage caused by the cyst. He was treated for his Crohn’s exacerbation and discharged from the hospital with no neurological side effects.
The author explains the case in this podcast:
References:
- Greenfield JP, Souweidane MM. Endoscopic management of intracranial cysts. Neurosurg Focus. 2005:19(6):E7.
- Monteagudo A, Timor-Tritsch IE. Prenatal diagnosis of CNS anomalies other than neural tube defects and ventriculomegaly. UptoDate. October 2014. Accessed December 2014.
- Malatt C, Sawaideh M, Chao C, et al. Head computed tomography in the emergency department: a collection of easily missed findings that are life-threatening or life-changing. J Emerg Med. 2014;47(6):646-659.
- Suthar PP, Patel JJ, Chetan M, Patel NA. Congenital porencephaly in a new born child. J Clin Diagn Res. 2014;8(11):RJ01-RJ02.
- Douzenis A, Rizos EN, Papadpooulou M, et al. Porencephaly and psychosis: a case report and review of the literature. BMC Psychiatry. 2010;10:19.