
Empowerment, Engagement, and Shared Decisions in the Real World of Clinical Practice
ABSTRACT: To meet the demands of a growing pay-for-performance healthcare system, clinicians must meet the challenges of assisting chronically ill patients to improve outcomes and participate in preventive health activities, while decreasing costs and creating a patient-centered environment. This article offers practical insight and strategies for cultivating involvement and self-management through empowerment, engagement, and shared decision-making. The authors discuss these concepts specifically for diabetes care organization and delivery, but these strategies can be broadly applied to other chronic diseases and preventive healthcare practices.
“Insanity: doing the same thing over and over again and expecting different results.” —Albert Einstein
As you enter your office and glance at your schedule, you see Ms Smith will be your first patient of the day. You immediately look around to see if there is anyone else available to see her. Although she is always pleasant and agreeable, you know that this visit will be much the same as all of the previous visits. You will give her the same evidence-based advice that you always do—stop smoking, lose weight, eat healthier, exercise more, take your medicine—and she will smile and agree, but in your heart you know that nothing will change because it never does. You’ve tried telling her about what can happen if she does not be more compliant; you’ve scolded her, praised her efforts, and sent her to the dietitian, but nothing has worked. On the one hand, you feel angry and frustrated that you can’t motivate Ms Smith, but on the other hand, you also feel as though you have failed at the end of each visit. If only you could get her to change and do what you know she should.
Does this sound familiar to you? If so, you are not alone. Addressing issues of adherence, compliance, and motivation are often identified as topics of great interest by providers when asked to identify continuing education needs. With the growth of pay-for-performance programs, healthcare providers are under more scrutiny than ever before to achieve designated outcome measures. There is more to do and less time to do it. Yet, many healthcare providers spend their time repeating the same messages in the same way and, not surprisingly, getting the same result. To help reduce these feelings of frustration or stress, this article gives an overview of different strategies and approaches that clinicians can use in order to create collaborative, effective relationships with their patients—and get a different result.
The Problem of Compliance
Patient compliance first appeared as a heading in Index Medicus in 1975. Since that time there has been a proliferation of studies on this topic as the number of patients with chronic illnesses continues to increase. Using diabetes as an example, there are more than 6000 articles for diabetes compliance and more than 4000 for diabetes adherence in Index Medicus.
It is clear that patients do not always follow the good advice we provide. The DAWN1 (Diabetes Attitudes, Wishes and Needs) study showed that self-reported, self-management behaviors were poor, particularly in the areas of diet and exercise.1 Out of more than 5000 participants with diabetes included in the study, only 19.4% of participants with type 1 diabetes and 16.2% with type 2 diabetes reported that they completely carried out all of the recommendations provided by their healthcare professionals. More than 2000 generalist and specialist providers who were included in the study rated patient behaviors even lower, with only 7.3% estimating that their typical type 1 patient and only 2.9% estimating that their typical type 2 patient was completely compliant with their recommendations.1 In the expanded and more recent DAWN2 study, self-reported behaviors continued to be low.2 In this study, more than 8000 patient participants indicated that following self-care advice was most common for medication and diet, and less common for glucose monitoring, physical activity, and foot examination.
In terms of medication-taking, rates for diabetes medications range from 60% to 90%.3 One study reported a 60.3% prevalence of statin continuation at 1 year and 48.8% at 5 years, with similar rates for beta-blockers and angiotensin-converting-enzyme inhibitors.4 It is clear that diabetes self-management is less than optimal in all aspects of the therapeutic regimen and has a large impact on outcomes.
Whose Problem Is It?
Over the years, patients and providers have blamed each other for this problem. “My doctor only cares about my numbers” and “My doctor doesn’t listen” are issues commonly voiced by patients. “My patients won’t do…”, “I don’t have time”, and “My patients aren’t motivated” are commonly voiced by physicians. But, in reality, neither patient nor physician is to blame. As healthcare professionals, we are typically trained in acute care settings and taught to feel responsible for our patients and their outcomes. But chronic disease care is different because the vast majority of the care is provided by the patient and is outside of the provider’s control. We have not been trained to respond to chronic illness, which requires proactive, coordinated care.
But our patients are also not to blame. Multiple studies have shown that patients feel a great deal of emotional distress at the time of the diagnosis of diabetes.1,2,5 A study by Fisher et al6 found high levels of diabetes-related distress in a sample of patients with type 2 diabetes (prevalence rates, 18% to 35%; 18-month incidence rates, 38% to 48%). In DAWN1, 85.2% of patients reported a high level of diabetes-related distress, including feelings of shock, guilt, anger, and anxiety at the time of diagnosis. Even 15 years after diagnosis, nearly 43% of patients continued to experience problems of living with diabetes, including fear of complications and both social and psychological burdens of self-care.1 These results were similar in DAWN2; while diabetes-related distress was reported by 44.6% of the patient participants, only 23.7% reported that their healthcare team asked them how diabetes impacted their life.2 Although it may seem less important than medications and other aspects of care, diabetes-related distress has a profound influence on outcomes and health behaviors. Some studies show that diabetes-related distress is linked to higher HbA1c levels and poor self-management.5,7
What does this all mean? When healthcare providers are trained in acute care settings, they are usually taught to be lifeguards. But no matter how good we are at being lifeguards, it just does not work for chronic diseases that are largely self-managed. In caring for chronic diseases, our job is to teach people to swim. One evidence-based approach to working more effectively with patients who have chronic illnesses is patient empowerment.
Patient Empowerment and Diabetes
The term patient empowerment was introduced in the diabetes literature in 19918 and has since been effectively incorporated into a variety of care and educational programs.9 Funnell et al8 defined empowerment in 1991 as “helping patients discover and develop their inherent capacity to be responsible for their own lives and gain mastery over their diabetes.” However, the concept of empowerment is often widely applied to other chronic diseases to describe how providing support, strategies, skills, knowledge, and responsibility can positively affect health and quality of life outcomes. The empowerment approach is based on 3 characteristics that differentiate diabetes and other chronic diseases from acute illnesses3,10:
1.The choices that have the greatest effect on metabolic and other outcomes are made by patients, not healthcare professionals.
2.Patients are in control of their self-management.
3.The consequences of self-management decisions accrue first and foremost to patients; thus, it is both their right and responsibility to be the primary decision-makers.
Patient empowerment is based in self-determination theory, which states that patients are more likely to make and sustain behavioral changes if they are personally meaningful and relevant.11 This theory further indicates that we all have basic needs for autonomy support (ie, for our priorities, needs, and feelings), relevant information (ie, for decision-making), competence (ie, self-efficacy), and relatedness (ie, feeling understood). Of these needs, the two most important for clinicians to provide in order to enhance patients’ self-directed behavior are relatedness and autonomy support.12
Empowerment
Empowerment is an essential component of patient-centered care, as it involves creating a collaborative partnership with patients and engaging in shared decision-making by assessing and incorporating their capacities, desires, needs, values, and barriers.8,13,14 Effective communication is key to this approach. While the clinical recommendations we provide are generally based on scientific evidence, the communication methods we use to convey that information are often based on personal style and experience. However, there is evidence demonstrating that effective communication by healthcare providers can improve medication-taking as well as other behaviors.9,13
One of these strategies is Ask, Listen, Empathize—a nondirective communication style based on active listening.15 With this approach, the healthcare professional asks questions to elicit the patient’s concerns and self-management struggles and barriers, and actively listens to the patient’s responses without offering opinions, criticism, or advice, while encouraging further reflection and discussion. The goal is to help patients understand the issue and identify personally meaningful and relevant solutions.15-17 These solutions are then used as the basis for self-determined behavioral goals and self-identified actionable steps to attain those goals. Other more complex approaches, such as motivational interviewing, use similar strategies, but a discussion of these other approaches is beyond the scope of this article.
It is important to keep in mind that the goal of empowerment-based communication is not to ensure that patients comply with the goals and recommendations of the healthcare provider. Rather, the goal is for patients to actively and effectively participate in their care and make informed decisions about both therapeutic and self-management recommendations. It is important to keep in mind that while physicians have scientific expertise, patients are the foremost experts on themselves and what is consistent with their lives, resources, and experiences.14
Patient Engagement
Patient engagement is an ethical approach consistent with patient-centered care and empowerment that places responsibility not only on patients, but also on health professionals, care organizations, and delivery systems.18 Patients who are actively engaged in their healthcare and self-management have or seek the understanding, knowledge, and skills to promote their own health and participate in their own healthcare.18 The DAWN2 study showed that people with diabetes do not believe they are actively engaged by healthcare providers and that diabetes self-management education and ongoing support are generally not available.2 While less than half of the patients were referred for diabetes education, more than 80% of those who attended educational sessions found them helpful in DAWN2.
Shared Decision-Making
Shared decision-making is a cost-effective approach to care that is designed to fully inform patients about the risks and benefits of available treatments and ensure their participation in treatment decisions. Shared decision-making is particularly relevant for improving medication use.19 A recent review of more than 86 clinical studies indicated that the use of evidence-based decision support aids improves patients’ knowledge of options, provides them with more accurate expectations of possible benefits and harms, motivates them to participate more fully in decision-making, helps them make choices more closely related to stated values, and overall improves communication with healthcare providers.20
It is important to keep in mind that there are no magic phrases or strategies you can use with patients like Ms Smith, and you cannot truly motivate another person for long-lasting behavior change. However, there are practical strategies for effective interaction that can be done in the context of a routine clinical visit that will not extend its length. For example, you can create a shared agenda by using a short form in the clinic waiting room that asks patients to indicate the area of greatest concern or difficulty, why that is an issue for them, their feelings about the issue and what they would like you to do to address the issue during the visit.21,22 You can also involve patients in decision-making and use the teach-back method,23 which engages patients by asking them to explain, in their own words, their understanding of what occurred during the visit. This method helps clinicians check for patient understanding and clarify any instructions, if needed. In addition, you can set a collaborative, behavioral goal by asking patients to identify one behavioral step they will take toward better managing their health.14
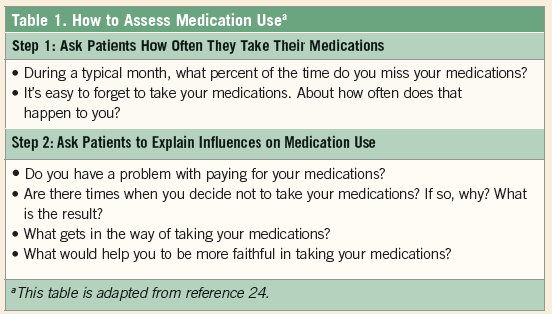
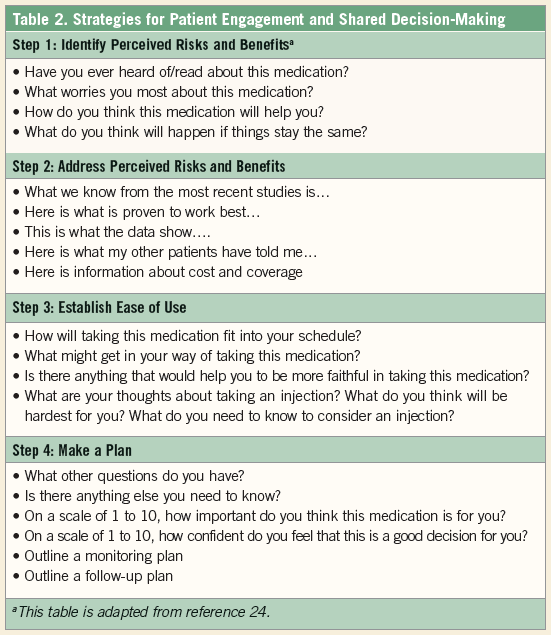
Table 124 outlines questions that clinicians can ask patients to assess their current medication use during a clinical visit. Asking patients to identify the percentage of medications missed during the previous month has been shown to be consistent with more precise methods of monitoring medication use.25 Table 224 outlines strategies to engage patients in shared-decision making and provide them with the information they need to actively participate and make informed decisions about their health.
Working With Ms Smith
Let’s go back to our example of Ms Smith. As you go into the room, you decide to take a new approach with Ms Smith with the hope of having a more productive encounter that will result in improved outcomes for her. Instead of focusing on her numbers and lack of compliance with your plan, you decide instead to focus on her issues and concerns.
Setting the Agenda
After greeting Ms Smith, you let her know that while you have some items on your agenda that you need to accomplish, you want to begin by hearing what is on her agenda for the visit. You start by asking her what has been hardest for her or her area of greatest concern since the last visit. She says she is having difficulty paying for her medications and more nutritious foods because she is recently separated from her husband. She also tells you that her son’s asthma has become more severe, resulting in several emergency department visits and more costly therapies. As a result, she is experiencing greater stress, which may be causing the increase in her A1c level. You express concern for her situation and ask if she would like a referral to a community resource that includes counseling and social worker support, to which she agrees.
Engagement and Shared Decision-Making
As the visit continues, you ask her about her medication use. You let her know that while a change in her treatment may be needed, the first step would be for her to take her current medications more routinely and monitor more frequently. She is currently taking metformin and a sulfonylurea, both of which are generic medications so that payment is not an issue, however, her coverage for glucose monitoring strips is limited. In addition, she says that the numbers are always good when she checks before breakfast and do not change, so she has not seen much point in paying for testing strips. You ask her if she has enough strips and would be able to do more intensive monitoring (6-8 times/day) for just 3 days in the next 2 weeks to give both of you a better idea of how the medications are working. After she agrees, you discuss targets for those readings, when she will do the testing, and when she will call your office with the results.
Teach-back and Goal-Setting
As you get ready to close the visit, ask Ms Smith to say in her own words what you have discussed. You then ask her to tell you one thing she will do differently to better care for her diabetes and health. She tells you that she knows her smoking is probably triggering some of her son’s asthma attacks, so she has decided that she will talk with the counselor at the community resource about smoking cessation strategies.
Reflecting on the Visit
As you leave the room after your encounter, you may still feel somewhat frustrated that not all of your goals for Ms Smith have been achieved. However, you feel better about the interaction and that it did not take any more time than your usual visit with her. You are also more hopeful that she may actually begin to make some of the changes she identified that will benefit her quality of life, overall health, and diabetes outcomes.■
Disclosures: This paper was supported in part by grant number P30DK092926 (MCDTR) from the National Institute of Diabetes and Digestive and Kidney Diseases.
References:
1. Skovlund SE, Peyrot M, DAWN International Advisory Panel. The Diabetes Attitudes, Wishes, and Needs (DAWN) program: a new approach to improving outcomes of diabetes care. Diabetes Spectrum. 2005;18(3):136-142.
2. Nicolucci A, Kovacs Burns K, Holt RI, et al; DAWN2 Study Group. Diabetes Attitudes, Wishes and Needs second study (DAWN2): cross-national benchmarking of diabetes-related psychosocial outcomes for people with diabetes [published correction appears in Diabet Med. 2013;30(10):1266]. Diabet Med. 2013;30(7):767-777.
3. Rubin RR. Adherence to pharmacologic therapy in patients with type 2 diabetes mellitus. Am J Med. 2005;118(suppl 5A):27S-34S.
4. Blackburn DF, Dobson RT, Blackburn JL, Wilson TW, Stang MR, Semchuk WM. Adherence to statins, beta-blockers and angiotensin-converting enzyme inhibitors following a first cardiovascular event: a retrospective cohort study. Can J Cardiol. 2005;21(6):485-488.
5. Fisher L, Glasgow RE, Strycker LA. The relationship between diabetes distress and clinical depression with glycemic control among patients with type 2 diabetes. Diabetes Care. 2010;33(5):1034-1036.
6. Fisher L, Hessler DM, Polonsky WH, Mullan J. When is diabetes distress clinically meaningful? Diabetes Care. 2012;35(2):259-264.
7. Reddy J, Wilhelm K, Campbell L. Putting PAID to diabetes-related distress: the potential utility of the Problem Areas in Diabetes (PAID) scale in patients with diabetes. Psychosomatics. 2013;54(1):44-51.
8. Funnell MM, Anderson RM, Arnold MS, et al. Empowerment: an idea whose time has come in diabetes education. Diabetes Educ. 1991;17(1):37-41.
9. Marrero DG, Ard J, Delamater AM, et al. Twenty-first century behavioral medicine: a context for empowering clinicians and patients with diabetes: a consensus report. Diabetes Care. 2013;36(2):463-470.
10. Funnell MM, Anderson RM. Patient empowerment: a look back, a look ahead. Diabetes Educ. 2003;29(3):454-564.
11. Deci EL, Eghrari H, Patrick BC, Leone DR. Facilitating internalization: the self-determination theory perspective. J Pers. 1994;62(1):119-142.
12. Ng J, Ntoumanis N, Thogersen-Ntoumani C, et al. Self-determination theory applied to health contexts: a meta-analysis. Perspect Psychol Sci. 2012;7(4):325-340.
13. Lyles CR, Schillinger D. Patient–provider communication and diabetes medication adherence: where do we go from here? Diabetes Management. 2013;3:183-188.
14. Funnell MM, Anderson RM. Empowerment and self-management education. Clin Diabetes. 2004;22(3):123-127.
15. Anderson RM, Funnell MM. The Art of Empowerment: Stories and Strategies for Diabetes Educators. 2nd ed. Alexandria, VA: American Diabetes Association; 2005.
16. Anderson B, Funnell MM, Tang TS. Self-management of health. In: The Art and Science of Diabetes Self-Management Education. Mensing C, ed. Chicago, IL: American Association of Diabetes Educators; 2006:43-46.
17. Anderson RM, Funnell MM. Patient empowerment: myths and misconceptions. Patient Educ Couns. 2010;79(3):277-282.
18. Danis M, Soloman S. Providers, payers, the community, and patients are all obliged to get patient activation and engagement ethically right. Health Aff (Millwood). 2013;32(2):401-407.
19. Veroff D, Marr A, Wennberg DE. Enhanced support for shared decision-making reduced costs of care for patients with preference-sensitive conditions. Health Aff (Millwood). 2013;32(2):285-293.
20. Stacey D, Legare F, Col NF, et al. Decision aids to help people who are facing health treatment or screening decisions. Cochrane Database Syst Rev. 2014;1:CD001431.
21. Diabetes concerns assessment form. Michigan Diabetes Research and Training Center, University of Michigan Health System website. http://www.med.umich.edu/mdrtc/profs/index.htm#conc. Accessed March 25, 2014.
22. Anderson RM, Patrias R. Getting out ahead: the diabetes concerns assessment form. Clin Diabetes. 2007;25(4):141-143.
23. Kaplan SH, Greenfield S, Ware JE Jr. Assessing the effects of physician-patient interactions on the outcomes of chronic disease [published correction appears in Med Care. 1989;27(7):679]. Med Care. 1989;27(suppl 3):S110-S127.
24. Funnell MM. Engaging the patient in diabetes self-management. J Fam Pract. 2013;62(12 suppl CME):S20-S26.
25. Gonzalez JS, Schneider HE, Wexler DJ, et al. Validity of medication adherence self-reports in adults with type 2 diabetes. Diabetes Care. 2013;36(4):831-837.
Martha M. Funnell, MS, RN, CDE is an associate research scientist in the department of medical education at the University of Michigan Medical School.
Robert M. Anderson, EdD is professor emeritus in the department of medical education at the University of Michigan Medical School.
Gretchen A. Piatt, MPH, PhD is an assistant professor in the department of medical education at the University of Michigan Medical School.