
An Elderly Woman with Altered Mental Status and Hypothermia
An 88-year-old woman is transferred from a nursing home due to an altered mental status and hypothermia.
History
Her baseline status is very poor. She has multi-infarct dementia caused by multiple strokes in the past. She is essentially bed-bound and has sustained frequent hospital admissions for dehydration, decubitus care, and urinary tract infections.
At baseline, she is conscious and easily arousable. In the last 24 hours, she was noted to be far less arousable and her most recent temperature was <95°C—the lower limit of the thermometer at the nursing home.
Physical Examination
On admission, the patient was obtunded and minimally arousable. She responded to painful stimuli. A properly calibrated rectal temperature was recorded as 90°F (32°C). Her mucosae were dry.
A cardiac exam revealed an irregular rhythm at 60 ventricular beats per min. A 2 cm sacral decubitus was noted.
Laboratory Tests
Pertinent lab findings revealed normal troponins, but an electrocardiogram showed atrial fibrillation, which is a new finding for this patient. A complete blood count revealed a white blood count of 16,000 with a left shift. A metabolic panel noted sodium at 156 meq/L, blood urea nitrogen at 42 mg/dL, and creatinine levels at 1.7 mg/L. Urinalysis showed concentrated urine with >30 white blood cells per high power field.
Treatment
She was started on warmed fluids, specifically 0.45% saline and renally-adjusted vancomycin and gentamycin. A warming blanket was applied.
Which of the following is the most appropriate statement about the presented patient’s condition?
A. Her acute prognosis is more related to her underlying condition than the hypothermia.
B. Control and reversal of the atrial fibrillation is the main determinant of her prognosis.
C. Optimal acute therapy is initiation of rewarming with extracorporeal membrane oxygenation (ECMO).
D. She will require either a dialysis or a ECMO-related maneuver to obtain a rewarming rate faster than 2°C per hour.
(Answer and discussion on next page)
Correct Answer: A. Her acute prognosis is more related to her underlying condition than the hypothermia.
The major point of emphasis in this case is that the patient has an extremely low core body temperature or accidental hypothermia. The precise definition is a core temperature <35°C/95°F without intent. The patient can then be further classified into 1 of several subcategories:
• Primary hypothermia describes an otherwise healthy person who is exposed to excessive cold and cannot produce adequate heat to maintain core body temperature. This is generally the case with classic cold exposures, such as snow catastrophes and cold water drownings.
• Secondary hypothermia is a situation when ill persons are unable to sustain a core body temperature even in a warm environment. A wide variety of medical conditions are associated with secondary hypothermia, including impaired thermoregulation (eg, anorexia nervosa, cerebrovascular accident [CVA], CNS trauma, and pharmalogic effects), endocrine failure (eg, hypoadrenalism and hypopituitarism), insufficient energy (eg, extreme physical exertion, hypoglycemia, and starvation), increased heat loss as with burns, and other clinical states (eg, carcinomatosis, overwhelming bacterial infections, and shock).1,2
Diagnosis
Our patient was diagnosed with secondary hypothermia. She displayed several medical complications, including multiple CVAs, urine and decubitus infections, and septicemia. Thus, the presence of hypothermia is not at all a surprise and in fact points to extent and serious nature of her comorbidities.
Treatment
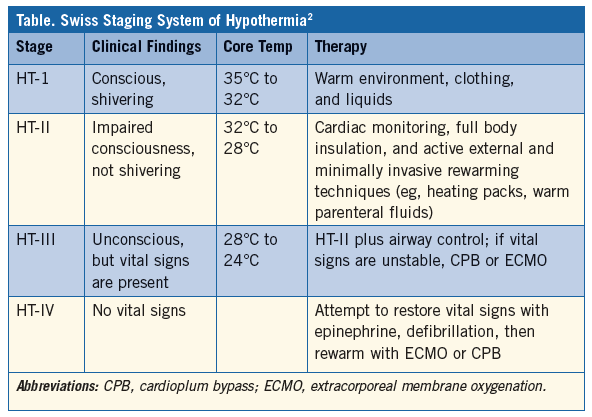
The so-called Swiss staging system of hypothermia presents a useful paradigm of the extent and associated findings of the hypothermia, with suggested therapy guidelines for each (Table).1 By clinical signs and temperature, our patient is at level HT-II, so can be managed with minimally invasive rewarming techniques; therefore, Answers C and D are considered too aggressive and not required here. Furthermore, Answer D is incorrect on the facts. It is true that the more aggressive and invasive rewarming techniques are capable of faster rewarming rates (eg, venovenous extracorporeal membrane oxygenation 4°C per hour). However, the less invasive treatments are quite capable of rewarming rates >2°C per hour (eg, active external up to 3.4°C per hour).2
Research suggests that the prognosis of properly treated hypothermia in an appropriate facility is quite good; survivorship and preserved organ function approaches 100% in HT-II patients.3,4 Unstable vital signs and cardiac arrest cases fare far worse.3,4 Good results accrue in primary cases, when the patients were healthy before the event. Morbidity and mortality in secondary cases, even the lesser levels of HL-I and HL-II, is much worse. In these situations, death is often caused by the underlying condition rather than the hypothermia.1,2 Answer A is the correct answer.
Note: Despite the ominous influence of malignant ventricular arrhythmias on outcome, atrial fibrillation is very common once the core temperature is below 32°C/90°F and is not a problematic marker in hypothermia; thus, Answer B is incorrect.
Outcome of the Case
Active external and minimally invasive rewarming techniques, specifically maintaining the horizontal position, creating a warm environment with blankets, and the administration of warm parenteral fluids, were put in place. By day 2, her core temperature had risen to 95°F (35°C). Blood cultures were reported as positive for enterococcus and appropriate antibiotic adjustments were made.
However, soon thereafter, progressive multi-organ failure ensued, including acute renal failure and hypotension. The family switched to comfort care measures only and she died peacefully on day 5.
Ronald Rubin, MD, is a professor of medicine at Temple University School of Medicine and chief of clinical hematology in the department of medicine at Temple University Hospital, both in Philadelphia, PA.
References:
1.Danzl DF, Pozos RS. Accidental hypothermia. N Eng J Med. 1994;331(26):1756-1760.
2.Brown AJ, Brugger H, Boyd J, Paal P. Accidental hypothermia. N Eng J Med. 2012;367(20):1930-1938.
3.Walpoth BH, Walpoth-Asian BN, Mattle HP, et al. Outcome of survivors of accidental deep hypothermia and circulatory arrest treated with extracorporeal blood warming. N Eng J Med. 1997;337(21):1500-1505.
4.Kornberger E, Schwarz B, Lindner KH, Mair P. Forced air surface rewarming in patients with severe accidental hypothermia. Resuscitation. 1999;41(2):105-111.