
Effect of Thyroid Dysfunction on Response to Warfarin
Many factors—eg, dietary vitamin K, age, other drugs, pharmacogenetics, and diseases—affect an individual’s response to warfarin.1 While many clinicians appropriately focus on drug interactions and dietary vitamin K when prescribing warfarin, it is quite easy to forget to assess the effect of disease states on this vitamin K antagonist. Among diseases that are well-documented to have a clinically relevant effect on response to warfarin are hyperthyroidism and hypothyroidism.2-11
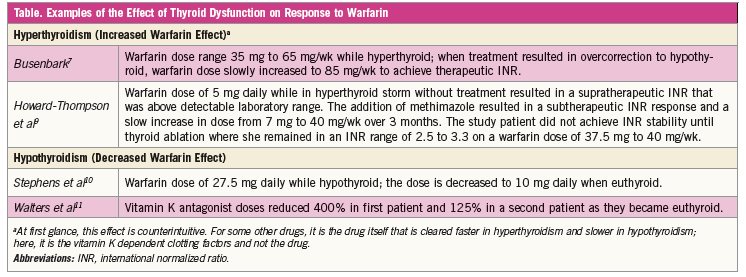
Hyperthyroidism
Hyperthyroidism increases response to warfarin by increasing catabolism of vitamin K dependent clotting factors.2 Several reports have documented elevated prothrombin time and international normalized ratio (INR) in patients receiving warfarin therapy while in the hyperthyroid state.3-9 A recent report extensively documented enhanced response to warfarin in a patient with Graves disease, followed by decreased response as the patient’s thyroid function returned to normal.9 Anticipate reduced warfarin dose requirements with need for dose adjustments as the patient becomes euthyroid.4-9 To help ensure safe and effective therapy, frequent monitoring of the INR is required.
Hypothyroidism
Hypothyroidism decreases the effect of warfarin likely by reducing the catabolism of vitamin K dependent clotting factors. This effect is documented to have marked clinical significance (Table).10,11 Expect increased warfarin dose requirements with need for dose adjustments and frequent monitoring of the INR as the patient returns to normal thyroid function.10,11
When clinicians see patients receiving long-term stable thyroid hormone and warfarin therapy, and the patients are now euthyroid, there should be no problem regarding that aspect of anticoagulation therapy. Difficulty in warfarin dosing is during the period of thyroid dysfunction, and close monitoring of the INR is essential.
Timothy Self, PharmD, is professor of clinical pharmacy at the University of Tennessee Health Science Center and program director, PGY2 Internal Medicine Pharmacy Residency, Methodist University Hospital in Memphis, TN.
Amanda Howard-Thompson, PharmD, BCPS, is an associate professor of clinical pharmacy and family medicine at the University of Tennessee Health Science Center in Memphis, TN.
References:
1.Ageno W, Gallus AS, Wittkowsky A, et al. Oral anticoagulant therapy—antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2012;141(2 suppl):e44S–e88S.
2.Loeliger EA, Van Der Esch B, Mattern MJ, Hemker HC. The biological disappearance rate of prothrombin, factors VII, IX and X from plasma in hypothyroidism, hyperthyroidism, and during fever. Thromb Diath Haemorrh. 1964;10:267-277.
3.McIntosh TJ , Brunk FS, Kölln I. Increased sensitivity to warfarin in thyrotoxicosis. J Clin Invest. 1970;
49:63a.
4.Vagenakis AG, Cote R, Miller ME, et al. Enhancement of warfarin induced hypoprothrombinemia by thyrotoxicosis. Johns Hopkins Med J. 1972;131(1):
69-73.
5.Self T, Weisburst M, Wooten E, et al. Warfarin induced hypoprothrombinemia. Potentiation by hyperthyroidism. JAMA. 1975;231(11):1165-1166.
6.Kellett HA, Sawers JS, Boulton FE, et al. Problems of anticoagulation with warfarin in hyperthyroidism. Q J Med. 1986;58(225):43-51.
7.Busenbark LA, Cushnie SA. Effect of Graves’ disease and methimazole on warfarin anticoagulation. Ann Pharmacother. 2006;40(6):1200-1203.
8.Akin F, Yaylali GF, Bastemir M, Yapar B. Effect of methimazole on warfarin anticoagulation in a case of Graves’ disease. Blood Coagul Fibrinolysis. 2008;
19(1):89-91.
9.Howard-Thompson A, Luckey A, George C, et al. Graves’ disease and treatment effects on warfarin anticoagulation. Case Rep Med. 2014;2014:
292468.
10.Stephens MA, Self TH, Lancaster D, Nash T. Hypothyroidism: effect on warfarin anticoagulation. South Med J. 1989;82(12):1585-1586.
11.Walters MB. The relationship between thyroid function and anticoagulant therapy. Am J Cardiology. 1963;11(1):112-114.