
Peer Reviewed
The Effect of Health Coaching and Population Health on Hypertension
Authors:
James J. Matera, DO; Kimberly Simers, MHA; and Alison Cleary, MSN
Citation:
Matera JJ, Simers K, Cleary A. The effect of health coaching and population health on hypertension. Consultant. 2017;57(10, Suppl.):S2-S4.
Approximately 30% of adults living in the United States have hypertension. With that ubiquity comes an increased risk for heart disease and other cardiovascular diseases, including stroke.1 The annual cost of treating hypertension in the United States approaches $50 billion for health care services, medications, and lost days of work associated with the condition and its sequelae.2 Certain underserved populations tend to have lower rates of hypertension, which can be attributed to the availability of community-based health care providers and programs that emphasize patients’ self-management of hypertension.3
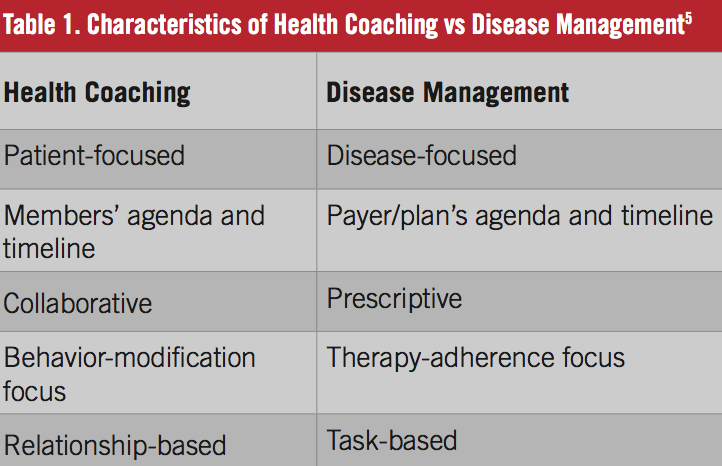
Health coaching has emerged over the last decade as an adjunct to clinical practice in several areas, and with various foundations and expectations. Its focus may be on education, navigation, advocacy, and direct management. Studies have shown some effectiveness to this approach; this likely will become more evident as the US health care system transitions from a pay-for-service model to a pay-for-performance model focusing on outpatient management, empowering patients in their care, and population health strategies (Table 1).5 Health coaching can be used successfully in various aspects of medical care, including the treatment of hypertension.4
This article reviews some of the findings from a New Jersey–based community medical center’s health coaching program in coordination with its primary care physicians.
BACKGROUND
The Eighth Joint Committee’s 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults (JNC 8)6 seemingly lowered the threshold for medical therapy in hypertension, and this remains a controversial point. Basically stated, pharmacologic therapy should be started in adults aged 60 years or older for a target blood pressure (BP) of 150/90 mm Hg or lower, and in adults younger than 60 years for a target of 140/90 mm Hg or lower. These measures still showed a decline in the rates of stroke, heart failure, and cardiovascular disease among patients with hypertension. In patients with type 2 diabetes mellitus, the target is 140/90 mm Hg or lower, regardless of age. In other at-risk adult populations (18 years and older), such as patients with chronic kidney disease, pharmacotherapy should be initiated to maintain a target BP of 140/90 mm Hg or below (a recommendation that is based on expert opinion and not evidence-based).
These guidelines have led to controversies about the management of hypertension in primary care practice, providing an opportunity for population health management with dedicated health coaches to enhance BP practice and lead to improved patient outcomes.6
Our practice in Freehold, New Jersey, developed a hypertension program in conjunction with the primary care physicians in CentraState Healthcare Partners (CHP), which is CentraState Medical Center’s physician hospital organization, and structured the program to include the following:
- Face-to-face meetings with health coaches
- Telephone contact with coaches and primary care providers
- Email correspondence, with the coach’s community lecture delivered midway through the program by a physician specializing in hypertension
Patient referrals to the program came from CHP primary care physicians; referrals were made using a printed checklist or an online protected application. The health coaches then contacted the patients to involve them in the health-coaching program.
Program OBJECTIVES
The objectives of the program were developed by the authors of this article and are as follows:
- To improve patients’ BP to target levels described in JNC 8
- To increase patients’ knowledge about hypertension risks and treatment plans
- To engage patients and empower them to pursue discussion about their treatment plan with their primary care provider
- To increase patients’ hypertension self-management skills
- To have patients achieve 75% adherence to home BP monitoring
- To ensure patients’ understanding of and adherence with medication regimens
- To ensure continued patient follow-up and communication with their primary care provider
PROGRAM PARTICIPANTS
The initial goal was to enroll 15 patients in a pilot program; the actual number of patients enrolled was 19. The participants’ average age was 61 years; 11 (58%) were men and 8 (42%) were women. Of the 19 participants, 17 (90%) were white and 2 (10%) were black or Hispanic. Seventeen participants (90%) were enrolled by way of direct referral from a CHP primary care physician; the other 2 (10%) self-enrolled through CentraState Medical Center’s Health Awareness Center. Each referring primary care physician was given a full report of the program’s results and the patients’ progress after completion.
RESULTS
At the completion of the 12-week health-coaching program, 13 participants (68%) had remained engaged with the program. Of this cohort, 100% had home BP monitors, and 7 (54%) had enrolled in additional programs offered by the Health Awareness Center. The average starting BP in this engaged cohort was 157/87 mm Hg, and the average ending BP was 136/81 mm Hg (Figure). After completion of the program, 9 participants (70%) had achieved a BP below 140/90, and 100% of these engaged patients self-monitored their BP at home. The results of this small pilot program included an average 13.3% decrease in systolic BP and an average 6.9% decrease in diastolic BP among the engaged cohort during the trial.

DISCUSSION
Self-measured BP monitoring is becoming an important adjunct to the care of patients with hypertension. Several national organizations, including the American Heart Association and the American Society of Hypertension, have encouraged the use of this technique for most patients with known or suspected hypertension.7
The advent of the Patient Protection and Affordable Care Act and the move of the health system toward a pay-for-performance model and away from a pay-for-service model require health care providers’ time to be being maximized in many areas of practice. The shortage of primary care providers in the United States will continue to add another layer of burden to already taxed primary care practices. This situation necessitates new and unique models to improve the delivery of health care and to optimize patient outcomes, while simultaneously driving down cost—the triple aim in today’s medicine.7
Population health will play an important role in the future of health care. Many organizations committed to population health are helping to build the infrastructure needed to support population health efforts, but collaboration across the continuum of care is essential to the success. To this end, our health care organization has committed itself to supporting aligned primary care practices by providing experienced registered nurse (RN) health coaches to perform patient outreach, motivational interviewing, and patient education, in order to engage and empower patients in managing their own chronic disease and mitigating risks to prevent disease progression. This collaboration helps primary care practices achieve improved clinical outcomes without having to absorb the direct costs associated with hiring personnel.
Health coaching is financially sustainable only if it can reduce total health care costs for payers (eg, Medicare, Medicaid, commercial health plans), and those payers share those savings with primary care practices, or if it can increase practices’ productivity in a fee-for-service payment model. Two organizations, using a 2 to 1 ratio of medical assistants to clinicians, have shown a positive business case for these additional support personnel by increasing revenue.8
Health coaches are experienced health educators with training from certifying bodies that emphasize core competencies such as ethics and standards of practice, active listening, communication styles, change readiness, goal setting, evidence-based practice interventions, telephone coaching, and motivational interviewing.9
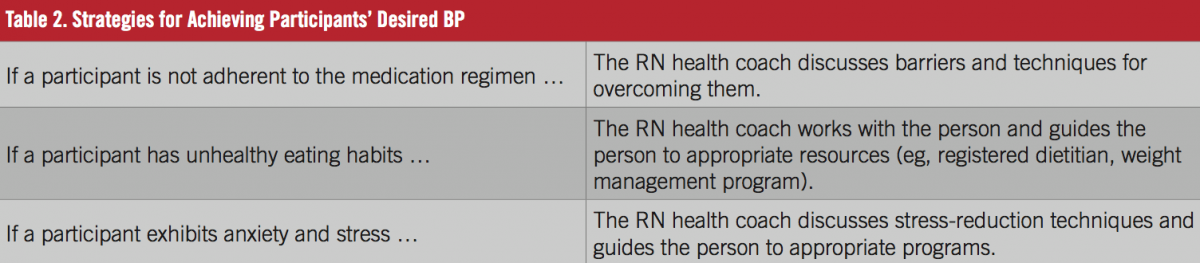
As a practical matter, our practice’s RN health coaches have faced a number challenges. After 3 unsuccessful attempts at outreach to a referred patient, outreach efforts ceased, and a patient follow-up feedback form was sent to the referring primary care provider. Approximately 28% of patients referred to the program never participated in it despite outreach attempts. Furthermore, the length of program was reduced from 12 weeks to 6 weeks after we observed that 50% of participants had achieved BP control or had lost interest in the program after week 6. Table 2 lists some of the strategies that our health coaches use to help patients achieve the desired BP.
CONCLUSIONS
Health coaching has been shown to improve sustainable clinical outcomes in hypertension and can be a helpful tool for primary care providers in today’s health care system.10 Our small cohort study demonstrates one way in which a community-based program can become a helpful adjunct to the primary care practice and strive to achieve the same goals of reducing cerebrovascular and cardiovascular events among its patients.11
While health coaching to improve patients’ self-management skills is an important component of an effective population health management strategy, such a program cannot succeed by itself. Health care systems and providers must work together to build a true culture of health in which all stakeholders are actively engaged in reducing costs and improving outcomes. In our experience, providers’ engagement occurs when they see the program’s positive impact on the health of their patients and feel a sense of partnership with program’s health coaches.
James J. Matera, DO, is an internal medicine and nephrology specialist at Nephrology-Hypertension Associates of Central Jersey in Freehold, New Jersey.
Kimberly Simers, MHA, is assistant vice president of integrative health at the CentraState Healthcare System in Freehold, New Jersey.
Alison Cleary, MSN, is manager of population health at the CentraState Healthcare System in Freehold, New Jersey.
REFERENCES:
- Centers for Disease Control and Prevention. High blood pressure frequently asked questions (FAQs). http://www.cdc.gov/bloodpressure/faqs.htm. Updated November 30, 2016. Accessed September 20, 2017.
- Davis KE. Expenditures for Hypertension among Adults Age 18 and Older, 2010: Estimates for the U.S. Civilian Noninstitutionalized Population. Rockville, MD: Agency for Healthcare Research and Quality; April 2013. Statistical Brief 404. https://meps.ahrq.gov/data_files/publications/st404/stat404.pdf. Accessed September 20, 2017.
- Brownstein JN, Chowdhury FM, Norris SL, et al. Effectiveness of community health workers in the care of people with hypertension. Am J Prev Med. 2007;32(5):435-447.
- Wolever RQ, Eisenberg DM. What is health coaching anyway?: standards needed to enable rigorous research. Arch Intern Med. 2011;171(22):2017-2018.
- Lawson KL, Jonk Y, O’Connor H, Riise KS, Eisenberg DM, Kreitzer MJ. The impact of telephonic health coaching on health outcomes in a high-risk population. Glob Adv Health Med. 2013;2(3):40-47.
- James PA, Oparil S, Carter BL, et al. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA. 2014;311(5):507-520.
- Pickering, TG, Miller NH, Ogedegbe G, Krakoff LR, Artinian NT, Goff D. Call to action on use and reimbursement for home blood pressure monitoring: executive summary: a joint scientific statement from the American Heart Association, American Society of Hypertension, and Preventive Cardiovascular Nurses Association. J Am Soc Hypertens. 2008;2(3):192-202.
- Bodenheimer T, Abramowitz S. Helping Patients Help Themselves: How to Implement Self-Management Support. Sacramento, CA: California Health Care Foundation; 2010. http://www.chcf.org/publications/2010/12/helping-patients-help-themselves. Accessed September 20, 2017.
- National Society of Health Coaches. NSHC health coach certification core competencies. https://www.nshcoa.com/core_competencies. Accessed September 20, 2017.
- Jacobson PD, Jazowski SA. Physicians, the Affordable Care Act, and primary care: disruptive change or business as usual? J Gen Intern Med. 2011;26(8):934-937.
- Sharma AE, Willard-Grace R, Hessler D, Bodenheimer T, Thom DH. What happens after health coaching? Observational study 1 year following a randomized controlled trial. Ann Fam Med. 2016;14(3):200-207.