
Education and Tools to Address the Rising Prevalence of Synthetic Cannabinoid Abuse
ABSTRACT: This article provides a thorough review of available literature to provide healthcare professionals with a better understanding of synthetic cannabinoid use and offer 3 strategies to enhance primary care screening and prevention efforts in clinical settings.
Public concern over synthetic cannabinoids has risen drastically in the past 3 years, mainly due to an increased prevalence of abuse. According to a 2011 report by the Institute for Social Research at the University of Michigan, synthetic cannabinoids are the second leading illegal drug of abuse among high school seniors.1 Other studies have suggested higher rates of use among certain at-risk populations—including lesbian, gay, bisexual, transgender, and queer and/or questioning (LGBTQ) community; active military personnel; and young men engaged in the criminal justice system.2-5 Both abuse and single episodes of use have led to severe clinical sequelae, including reports of hospitalizations for acute kidney failure, seizures, stroke, myocardial infarction, and psychosis, as well as reports of addiction leading to physical symptoms of withdrawal.
Because of this, most recent studies recommend increasing awareness among both healthcare providers and affected populations of the risks associated with synthetic cannabinoid use to enhance prevention, screening, and harm reduction efforts. Although such campaigns have been launched by the CDC and the United States military as well as by departments of health in cities such as New York and Washington, DC, no clear and concise strategies to inform and guide screening and prevention in clinical settings currently exist.6
This article proposes 3 strategies to enhance screening and prevention efforts in clinical settings:
• Identify at-risk populations and individual risk factors for synthetic cannabinoid use and abuse to create clear, targeted screening guidelines
• Create simple information points to guide medical professionals in the provision of patient education
• Disseminate information-driven materials designed with the above at-risk populations in mind
These efforts were successfully implemented at a satellite clinic serving LGBTQ adolescents age 16 to 24 years, one of the targeted high-risk populations identified through prior studies. Although a controlled study exploring the efficacy of these measures is not available, this project aims to serve as a model that can be implemented in other clinical arenas where synthetic cannabinoid use is of concern and as a foundation to build from as further research on this new and emerging substance of abuse evolves.
Synthetic Cannabinoids
Synthetic cannabinoids are laboratory-created compounds that mimic the effects of cannabis. They were initially created for research purposes in the 1970s, but their recent marketability has led to the production of many different compounds that have not been researched and are hard to track. The most commonly encountered strains include JWH-018 (also known as AM-678), JWH-073, JWH-200, CP 47,497 (also known as [C7]-CP 47,497), and (C8)-CP 47,497 (also known as cannabicyclohexanol).
These compounds are extremely potent agonists of cannabinoid receptors and have been found to have higher affinity to these receptors, which can lead to longer half-lives in some strains and can produce active metabolites.7 The increased affinity and potency of synthetic cannabinoids are thought to result in an exaggerated side effect profile compared with natural cannabis.7-9 Producers most often use an herb or a plant base that is then sprayed with a synthetic cannabis compound. Other toxic chemicals, such as clenbuterol, have also been found in these mixtures.10 Synthetic cannabinoids are often referred to as K2 (the street name most commonly used for synthetic marijuana in Harlem), Spice, Aroma, and Black mamba (Table 1).11-13
 Clinical Sequelae
Clinical Sequelae
The high that is experienced after smoking synthetic marijuana generally lasts 3 to 4 hours—as compared to 2 to 3 hours after smoking marijuana14—and has been associated with more negative effects. These effects are generally self-limiting and include tachycardia, paranoia, nausea, vomiting, dizziness, hallucinations, slurred speech, and drowsiness.15 As more strains have been created to evade regulations banning their distribution,7 ingestion has been linked to further serious sequelae (eg, seizures, acute renal failure, stroke, and myocardial infarction).10,16
In addition to the physical clinical sequelae, synthetic marijuana use has been associated with psychosis and an increased incidence of psychotic relapse for individuals with underlying mental illness.9 Forrester et al17 reported that cannabis-associated psychopathological syndrome was more likely to occur with synthetic cannabis use than with marijuana use (11.2% vs 2%, respectively).” This may be due to a lack of naturally occurring cannabidiol found in natural cannabis, which mitigates the neuropsychiatric effects of delta-9-tetra-hydrocannabinol in the endocannabinoid system, mainly paranoia and agitation.18 In addition, most strains of synthetic cannabis bind with a higher affinity to cannabinoid receptors than their natural counterparts, thereby having increased potency.7 This explains the increased frequency and level of agitation as well as the notable lack of behavioral control observed in psychosis secondary to synthetic versus natural marijuana use.19 Although psychosis is often self-limited, current research proposes that the varying metabolism of some strains of synthetic cannabis may have longer-term effects on brain function,7 and controlled case studies affirm the need for inpatient admission and long-term medication management for psychosis following synthetic cannabis ingestion.20 The pharmacologic effects of synthetic cannabis have also been linked to noted tachyphylaxis21 and possible physical dependence and withdrawal syndromes.22
Because of its toxic effects and psychologic sequelae, synthetic marijuana exposure accounted for 5230 reports to poison control centers in 2012 and 2643 calls in 2013.23 In 2011, 28,531 out of 2,460,000 substance abuse-related emergency department visits were linked specifically to synthetic cannabis use.24 The New York City Department of Health and Mental Hygiene issued a press release in July 2014 to warn New York residents about the risks associated with synthetic cannabis use after it noticed a 220% increase in emergency department visits related to use of this substance in 2014.25 The most notorious series of cases occurred in 2013 in Denver, CO, when 263 emergency department visits were logged in less than 1 month. Although most patients were treated and sent home, 15 people required ICU admission related to both neuro- and cardiotoxicity.26
Regulation and Forensic Toxicology
Synthetic marijuana was available for sale online in 2006, and the first specimen flagged the United States Drug Enforcement Administration (DEA) was in 2009.21 The Synthetic Drug Abuse Prevention Act of 2012,27 passed by Congress and signed by President Obama, permanently placed 5 strains of synthetic cannabis as Schedule I substances, which are regarded as the most dangerous class of drugs due to their high potential for abuse and potentially severe psychological and physical dependence.28 Seven other strains were temporarily listed as Schedule I substances that same year.29 The process of placing synthetic cannabinoids on the federal list of banned substances is difficult due to concerns regarding the interruption of scientific studies using these compounds and the rapid rate of novel substance emergence.8,29
Although certain strains of synthetic marijuana have been banned in the United States, it is still easily accessible online and can often be purchased in corner stores and at head shops. Vendors attempt to evade regulation by labeling packages as “not for human consumption.” Regulations differ by state and, in many cases, it appears that these regulatory standards have yet to filter down to individual retailers. In 2014, officials have begun to crack down on enforcement, with multiple DEA raids and local law enforcement investigations, resulting in over 150 arrests and the seizure of hundreds of thousands of bags of synthetic marijuana valued over $20 million.30
New strains are continuously hitting the market to avoid these regulatory standards. This constant stream of emerging strains has led to difficulty in establishing timely forensic toxicology screening to confirm use in the face of patients presenting to clinics, psychiatry departments, and emergency rooms with toxic symptoms. Beginning in 2010, however, laboratories began developing testing strategies that can identify metabolites and parent compounds using mass spectrometry.7 The Community Drug Early Warning System (CDEWS) Pilot Project used this technology successfully in its study to retroactively screen urine for 12 synthetic cannabinoid strains.5 It has just recently started being offered by clinical and forensic laboratories such as Quest Diagnostics,31 Ameritox,32 and NMS Labs.33 It has yet to be determined how urine toxicology screening can be integrated into practice.
Prevalence of and Risk Factors
In 2012, the National Institute on Drug Abuse reported that 11.3% of high school seniors in the United States smoked synthetic marijuana in the past year.34 Another study conducted at Georgia universities found that 14% of college students had used synthetic cannabis, and that the highest rates were encountered among LGBTQ individuals with 27% reporting having ever used synthetic cannabis.3 In all of the studies reviewed, over 90% of individuals who reported synthetic cannabinoid use also reported a history of marijuana use9,35-37 and between 77% and 84% reported a concomitant history of cigarette smoking.35,36
According to the CDEWS Pilot Project,5 between 19% and 37% of young men interacting with the criminal justice system near Washington, DC, and Richmond, VA, tested positive for synthetic cannabinoids. They found that synthetic cannabis was the only substance that was just as likely to be found in the systems of those who had tested negative for any other drug use as those who had tested positive. This type of study is used to provide drug forecasting to identify emerging substances of abuse in local communities and highlights the finding that synthetic cannabis use is often linked to the avoidance of having a positive urine toxicology screening.37
Another population that has been found to be at increased risk for synthetic cannabis abuse is active military personnel. A 2014 study funded by the Department of Defense found that synthetic cannabis was the most prevalently abused illicit substance, with 38% of active-duty United States Army personnel reporting use.4 Of those with prior histories of substance abuse and positive reporting of synthetic cannabis use, 68% met the criteria for dependence. The study also revealed that synthetic cannabis use was perceived by participants to be far more prevalent in this population than in the general public.
Public Perception
Despite the harms associated with its use, the rates of synthetic cannabis abuse remain elevated among at-risk populations. A 2012 study noted that 11% of respondents believed that Spice was “natural” and most participants thought that it was “generally safe for use.”15 Multiple studies have noted that, because it is still widely available in corner stores and it is not detectable on urine drug screen, it is still considered a “legal” high. In addition to the noted desirability of such a potent high, this availability and lack of detection on drug screen are 2 of the top reasons for continued use of synthetic cannabis despite the negative side effects.35,36

Strategies to Enhance Screening and Prevention Efforts in Clinical Settings
Almost all studies related to synthetic cannabinoid use have called for increased public awareness of this problem, which includes educating at-risk populations of the emerging drug’s risk profile and increasing healthcare provider vigilance in detecting and screening for synthetic cannabinoid use to provide targeted intervention strategies.
According to The National LGBTQ Task Force, between 20% and 40% of homeless youth identify as LGBTQ despite the fact that only 3% to 5% of the general population identifies as LGBTQ.38,39 A 1997 study reported that approximately 75% of homeless adolescents use marijuana.40 Rates of marijuana use among young men who have sex with men that have been kicked out of their homes have been found to be well above those of the normal population.41 In addition, homeless LGBTQ adolescents have been found to have increased mental health risks, including higher rates of major depression, anxiety, posttraumatic stress disorder, suicidality, disorderly conduct, and substance abuse.42,43 Homeless LGBTQ adolescents are particularly at risk not only for K2 abuse but also for the adverse effects on mental health and risk of psychiatric deterioration that is most commonly observed in vulnerable populations using synthetic cannabinoids.
The successful implementation of the model presented in this article into a primary care setting suggests that further research into preventive and screening strategies in high-risk clinical settings is warranted. Further research into treatment options must be pursued as well. No concrete guidelines to address the treatment of synthetic cannabinoid use and abuse currently exist. Suggested treatment for marijuana abuse, such as psychotherapy and incentive-driven methods, are lacking in data to substantiate their efficacy.6 Despite this, these methods may prove to be beneficial options for referral as we wait for more data in this field to emerge.
The development of prevention, education, screening, and treatment strategies for this emerging drug of abuse is an important component of healthcare maintenance for at-risk populations, especially adolescents and young adults, and should continue to be pursued.
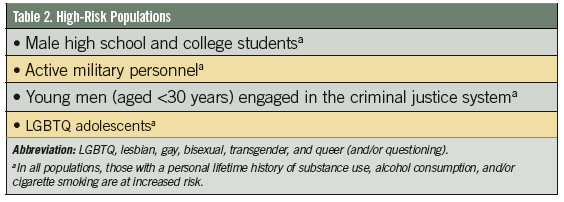
Methods
The aim of this review was to create and implement a model in a setting with a population particularly at risk for synthetic cannabis use and abuse. Based on the discussed literature review, a comprehensive list of at-risk populations was formulated (Table 2). From this list of at-risk populations combined with individual risk factors for synthetic cannabis use and commonly seen clinical presentations of synthetic cannabis intoxication, we then generated a set of targeted clinical screening recommendations (Table 3). In addition, a set of brief, comprehensive talking points for patient education that can be conducted during routine health screening was produced (Table 4) and a postcard aimed at raising awareness in at-risk populations in a marketable and information driven way was designed and disseminated among clients both in the clinic and the drop-in center at large.
This model was implemented at a satellite clinic located within a drop-in center in central Harlem serving homeless LGBTQ adolescents age 16 to 24 years. The drop-in center provides meals, clothing, mental health services, HIV testing and treatment, substance abuse support, career and educational counseling, mentoring, and intensive case management. It is part of a larger organization that provides emergency and long-term housing options for homeless LGBTQ youth. The drop-in center and the clinic are open 7 days per week and 3 days per week, respectively.
Using the screening guidelines in Table 3, all youth, with a particular focus on individuals with a positive history of substance use of any form, were asked about lifetime use of K2. Among those screened, all youth reporting a positive history of substance use or abuse were educated on synthetic cannabinoids using the key talking points, whether they reported a positive or negative history of synthetic cannabinoid use. In addition, youth presenting with signs and symptoms of possible synthetic cannabinoid toxicity were questioned about use. Of these, 3 youth that screened positively for synthetic cannabinoid use immediately prior to seeking care were transferred to the emergency department for further evaluation and supportive care. One of these individuals experienced nausea, vomiting, and tachycardia associated with extrapyramidal symptoms; another patient experienced nausea, vomiting, tachycardia, paranoia, altered mental status, and ataxia; and the third individual experienced an acute episode of psychosis.
Discussion
On-site case management staff and licensed therapists have reported an increase in dialogue about synthetic cannabinoids since the implementation of this model. Further, clients presenting to the clinic have engaged in discussions about K2 with other clients and staff in the waiting room after picking up the informative postcards. Due to a lack of ability to collect clear data on K2 use in the electronic medical records used in the clinic in which this model was implemented and time restraints in conducting the study, concrete data on the efficacy of this model could not be collected. However, clients who have screened positive for K2 abuse, including one who was sent from our clinic to the emergency department, have anecdotally mentioned the cessation of synthetic cannabinoid use after undergoing the screening and education provided with this model.
References:
- Johnston L, O’Malley P, Bachman J, Schulenberg J. Monitoring the future national results on adolescent drug use: overview of key findings, 2011. The University of Michigan Institute for Social Research. 2012 Feb. www.monitoringthefuture.org/pubs/monographs/mtf-overview2011.pdf. Accessed June 4, 2014.
- Bebarta VS, Ramirez S, Varney SM. Spice: a new “legal” herbal mixture abused by young active military duty personnel. Subst Abus. 2012;33(2):191-194.
- Stogner J, Miller BL. A spicy kind of high: a profile of synthetic cannabinoid users. J Subst Use. 2014;19(1-2):199-205.
- Walker D, Neighbors C, Walton T, et al. Spicing up military: use and effects of synthetic cannabis in substance abusing army personnel. Addict Behav. 2014;39(7):1139-1144.
- Wish E, Artigiani E, Billing A. Community drug early warning system: the CDEWS pilot project, Office of National Drug Control Policy. Executive Office of the President. 2013 Sep. www.whitehouse.gov/sites/default/files/finalreport_with_cover_09172013.pdf. Accessed May 10, 2014.
- Nyamathi A, Hudson A, Greengold B, et al. Correlates of substance use severity among homeless youth. J Child Adolesc Psychiatr Nurs. 2010;23(4):214-222.
- Seely KA, Lapoint J, Moran JH, Fattore L. Spice drugs are more than harmless herbal blends: a review of the pharmacology and toxicology of synthetic cannabinoids. Prog NeuroPsychopharmacology Biol Psychiatry. 2012;39(2):234-243.
- Harris CR, Brown A. Synthetic cannabinoid intoxication: a case series and review. J Emerg Med. 2013;44(2):360-366.
- Every-Palmer S. Synthetic cannabinoid JWH-018 and psychosis: an explorative study. Drug Alcohol Depend. 2011;117(2-3):152-157.
- Pourmand A, Armstrong P, Mazer-Amirshahi M, Shokoohi H. The evolving high: new designer drugs of abuse. Hum Exp Toxicol. 2014;33(10):993-999.
- Synthetic marijuana: street and shelf names. Rensselaer County Public Health Department. www.rensco.com/pdfs/Health/SynMar/Product%20Names%20of%20Synthetic%20Marijuana.pdf. Accessed August 5, 2014.
- K2–Spice. Partnership for Drug Free Kids. www.drugfree.org/drug-guide/k2-spice. Accessed June 4, 2014.
- Drug Fact Sheet: K2 or Spice. Drug Enforcement Agency. www.dea.gov/druginfo/drug_data_sheets/K2_Spice.pdf. Accessed October 1, 2014.
- Grotenhermen F. Pharmacokinetics and pharmacodynamics of cannabinoids. Clin Pharmacokinet. 2003;42(4):327-360.
- Vandrey R, Dunn KE, Fry JA, Girling ER. A survey study to characterize use of Spice products (synthetic cannabinoids). Drug Alcoh Depend. 2012;120(1-3):238-241.
- Brust JC. Spice, pot, and stroke. Neurology. 2013;81(24):2064-2065.
- Forrester MB, Kleinschmidt K, Schwarz E, Young A. Synthetic cannabinoid and marijuana exposures reported to poison centers. Hum Exp Toxicol. 2012;31(10):1006-1011.
- Muller H, Sperling W, Kohrmann M, et al. The synthetic cannabinoid Spice as a trigger for an acute exacerbation of cannabis induced recurrent psychotic episodes. Schizophr Res. 2010;118(1-3):309-310.
- Papanti D, Schifano F, Botteon G, et al. “Spiceophrenia”: a systematic overview of “spice”-related psychopathological issues and a case report. Hum Psychopharmacol. 2013;28(4):379-389.
- Van Der Veer N, Friday J. Persistent psychosis following the use of Spice. Schizophr Res. 2011;130(1-3):285-286.
- Wells DL, Ott CA. The “new” marijuana. Ann Pharmacother. 2011;45(3):414-417.
- Nacca N, Vatti D, Sullivan R, et al. The synthetic cannabinoid withdrawal syndrome. J Addict Med. 2013;7(4):296-298.
- American Association of Poison Control Centers. Synthetic marijuana data. 2014 Feb 28. https://aapcc.s3.amazonaws.com/files/library/Syn_Marijuana_Web_ Data_through_2.2014.pdf. Accessed May 10, 2014.
- The DAWN Report: Drug Related Emergency Department Visits Involving Synthetic Cannabinoids. Rockville, MD: Substance Abuse and Mental Health Services Administration, US Dept of Health and Human Services; 2012.
- Miller S. Health department warns New Yorkers of dangers of synthetic cannabinoids. New York City Department of Health and Mental Hygiene. July 27, 2014. www.nyc.gov/html/doh/html/pr2014/pr023-14.shtml. Accessed August 30, 2014.
- Rodgman C, Kinzie E, Leimbach E. Bad Mojo: use of the new marijuana substitute leads to more and more ED visits for acute psychosis. Am J Emerg Med. 2011;29(2):
- 232.
- AAPCC issues statement on the synthetic drug abuse prevention act. American Association of Poison Control Centers. July 11, 2012. www.aapcc.org/press/2. Accessed August 2014.
- United States drug enforcement association. Drug schedules. United States Department of Justice. www.dea.gov/druginfo/ds.shtml. Accessed July 2015
- Sacco L, Finklea K. Synthetic drugs: overview and issues for congress. Congressional Research Service. 2014. www.fas.org.ezproxy.cul.columbia.edu/sgp/crs/misc/R42066.pdf. Accessed August 14, 2014.
- Phillip A. DEA raids synthetic drug manufacturers in a major nationwide crackdown. The Washington Post. www.washingtonpost.com/news/post-nation/wp/2014/05/07/dea-raids-synthetic-drug-manufacturers-in-a-major-nationwide-crackdown. Accessed August 14, 2014.
- Testing for synthetic drugs. Quest Diagnostics. www.questdiagnostics.com/home/companies/ employer/drug-screening/drugs-tested/synthetics. Accessed September 30, 2014.
- K2 Spice drug test–synthetic marijuana urine drug testing. Ameritox Medication Monitoring Solutions. www.ameritox.com/k2-spice-drug-test-synthetic-marijuana-urine-drug-testing. Accessed August 28, 2014.
- K2, Spice and other synthetic cannabinoids testing. NMS Labs. www.nmslabs.com/services-forensic-k2-testing. Accessed August 28, 2014.
- Drug Facts: K2/Spice ("Synthetic Marijuana"). National Institutes on Drug Abuse. 2012 Dec. www.drugabuse.gov/publications/drugfacts/spice-synthetic-marijuana. Accessed June 3, 2014.
- Hu X, Primack BA, Barnett TE, Cook RL. College students and use of K2: an emerging drug of abuse among young persons. Subst Abuse Treat Prev Policy. 2011;6:16.
- Winstock A, Barratt M. Synthetic cannabis: a comparison of patterns of use and effect profile with natural cannabis in a large global sample. Drug Alcoh Depend. 2013;
- 131(1-2):106-111.
- Perrone D, Helgesen RD, Fischer R. United States drug prohibition and legal highs: how drug testing may lead cannabis users to Spice. DEPP. 2013;20(3):216-224.
- Sklar R. Fact sheet: homeless lesbian, gay, bisexual and transgender (LGBT) youth in New York. National Gay and Lesbian Task Force. 2007. www.thetaskforce.org/downloads/reports/fact_sheets/ HomelessYouthNewYork012507.pdf. Accessed May 30, 2014.
- Fact sheet: homeless lesbian, gay, bisxual and trandgender youth in New York Samhsa Homelessness Resource Center. http://homeless.samhsa.gov/resource/fact-sheet-homeless-lesbian-gay-bisexual-and-transgender-lgbt-youth-in-new-york-26485.aspx. Accessed July 2015.
- Greene JM, Ennett ST, Ringwalt CL. Substance abuse among runaway and homeless youth in three national samples. Am J Pub Health. 1997;87(2):229-235.
- Bruce D, Stall R, FataA, Campbell R. Modeling minority stress effects on homelessness and health disparities among young men who have sex with men. J Urban Health. 2014;91(3):568-580.
- Keuroghlian AS, Shtasel D, Bassuk EL. Out on the street: a public health and policy agenda for lesbian, gay, bisexual, and transgender youth who are homeless. Am Orthopsychiatry. 2014;84(1):66-72.
- Bhatty S, Wu W. Organic and synthetic cannabis use in adolescents. Pediatr Ann. 2013;42(1):31-35.