
A Collection of Men’s Health Issues
Epidermoid Cyst of the Testis
Joseph Anderson, MD, and Nathan C. Birch, MD
A 25-year-old man sought evaluation of a painless, palpable, left testicular mass that had been present for more than 1 year. There was no personal or family history of cryptorchidism or malignancy. A circumscribed mass was palpated within the anterior superior pole of the left testis. Initial laboratory test results were within normal limits.
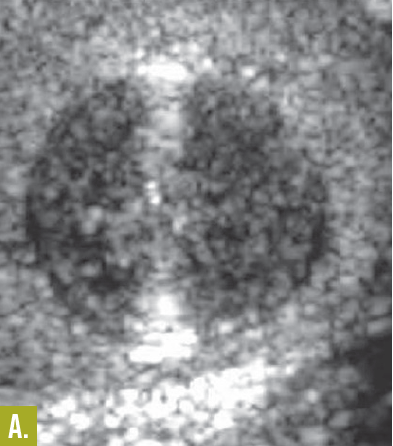
Laboratory testing. An ultrasonogram revealed a 1.6 x 1.2 x 1.2 cm cystic structure with alternating hypoechogenicity and hyperechogenicity that strongly suggested an epidermoid cyst. However, a carcinoma could not be ruled out. A period of monitoring with ultrasonographic examinations was observed for several months. This patient subsequently underwent a partial orchiectomy. Although a benign cyst was suspected, the surgeon opted for this procedure to exclude intratubular germ cell neoplasia. Pathologic examination revealed a well-circumscribed, white-tan, laminated lesion within unremarkable, red-brown testicular parenchyma. The largest dimension of the mass measured 1.6 cm. Microscopic examination confirmed the diagnosis of a benign epidermoid cyst.

Discussion. The physicians reported that epidermoid cysts comprise 1% of testicular masses.1 These well-circumscribed, solid masses, which most often occur in the second to fourth decades of life, are not associated with distant metastases or local recurrence.1-3 The cyst is composed of a fibrous wall lined with squamous epithelium and filled with keratin debris. The layering of this debris imparts the classic “onion skin” or “target” appearance on an ultrasonogram.4 Germ cell tumor can be ruled out by histologic examination.
Outcome of the case. Preoperative ultrasonographic evaluation that strongly suggests an epidermoid cyst can direct the therapeutic course toward lesion enucleation, which is a more conservative treatment than a radical orchiectomy. The patient’s recovery was uneventful and complete.
References:
1. Shah KH, Maxted WC, Chun B. Epidermoid cysts of the testis: a report of three cases and an analysis of 141 cases from the world literature. Cancer. 1981;47(3):577-582.
2. Malek RS, Rosen JS, Farrow GM. Epidermoid cyst of the testis: a critical analysis. Br J Urol. 1986;58(1):55-59.
3. Dieckmann KP, Loy V. Epidermoid cyst of the testis: a review of clinical and histogenetic considerations. Br J Urol. 1994;73(4):436-441.
4. Langer JE, Ramchandani P, Siegelman ES, Banner MP. Epidermoid cysts of the testicle: sonographic and MR imaging features. AJR Am J Roentgenol. 1999;173(5):1295-1299.
Pituitary Macroadenoma
M. Usman Chaudhry, MD
During a workup for dementia, a 77-year-old man was found to have a pituitary macroadenoma (21 x 17 x 25 mm) with suprasellar extension on a coronal-section MRI scan. The patient had hypertension and mild erectile dysfunction. He denied headaches, nausea, vision problems, weight changes, weakness, and polyuria. His medications included nifedipine, hydrochlorothiazide, and aspirin.

Physical examination. The patient’s blood pressure was 150/80 mm Hg. He had no cushingoid or acromegalic features. A left inferolateral visual field defect was noted by confrontation method. He had lipomatosis without gynecomastia, Tanner stage 4 hair distribution on inguinal and axillary regions, and normal-sized testicles. He had no hormonal deficiencies or excess; prolactin level was 11 µg/L (normal, 2 to 15 µg/L). The physician noted that pituitary tumors not associated with hormonal hypersecretion are termed “nonfunctional pituitary tumors.”
Discussion. They usually present with symptoms of mass effect, such as bitemporal visual field defect; headache; and palsy of cranial nerves III, IV, and VI. Most of these lesions are derived from gonadotroph cells and may produce luteinizing hormone or follicle-stimulating hormone, or subunits of these hormones.
In a patient who has a sellar mass, the diagnosis of nonfunctional pituitary tumor is usually made after prolactinoma, acromegaly, and Cushing disease have been ruled out clinically and biochemically. For lesions larger than 1 cm, neurosurgical removal is often necessary, and the pituitary cell origin is confirmed on histology. Medical therapy is not useful in most patients. Significant residual tumor is typically treated with radiation therapy.
Treatment. This patient’s tumor was excised; histopathologic analysis confirmed a nonfunctional adenoma. Six weeks after the operation, the patient’s morning cortisol level remained adequate, 454 nmol/L (it should be greater than 270 nmol/L for patients with pituitary disease); free thyroxine was 15.5 pmol/L (normal, 10.3 to 24.4 pmol/L); and total testosterone was 14.3 nmol/L (normal, 7.4 to 25.7 nmol/L).
Outcome of the case. Alpha subunit was not high, and he had no diabetes insipidus. A repeated coronal-section MRI scan of the pituitary showed residual tumor. The patient was referred for stereotactic radiosurgery.
Cutaneous Metastasis of Prostatic Adenocarcinoma
Emily Stevens, MD, Andrew Dubois, MD, and Ivan Damjanov, MD, PhD
This lesion appeared in the right groin of a 60-year-old man and slowly enlarged over a month. Two years before this evaluation, he underwent total prostatectomy with lymph node dissection for prostate carcinoma. Metastatic disease was found in a resected lymph node, and he underwent multiagent chemotherapy.

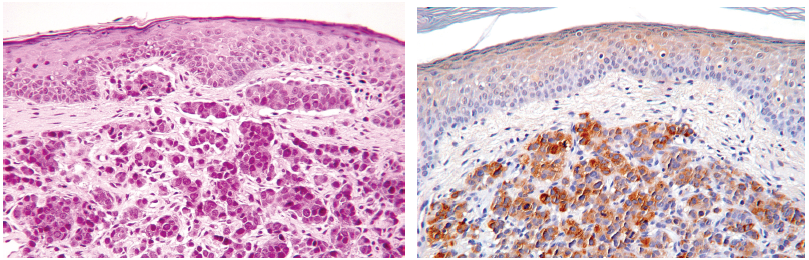
Laboratory testing. Histopathological examination of a shave biopsy specimen from the nodule revealed adenocarcinoma in the dermis with an intact overlying epidermis. In view of the patient’s history, metastasis from the primary carcinoma in the prostate was considered the most likely diagnosis. Immunohistochemical staining with the antibody to prostate-specific antigen confirmed prostatic adenocarcinoma.
Discussion. Carcinoma of the prostate tends to metastasize to many organs, including bone, lung, liver, and adrenal glands.1 However, metastases to the skin are rare; they occur in fewer than 1% of patients with metastatic disease.2 Most of these metastases are located on the skin of the abdomen, especially the suprapubic area, the anterior thighs, and the groin.
Prostatic carcinomas that have metastasized to the skin are associated with a poor prognosis; death from disseminated cancer generally occurs within 1 year.3
Outcome of the case. This patient died within 6 months of the skin biopsy.
References:
1. Nebesky JM, Abangan DL, Kauffman CL. Infiltrated groin plaque in an 81-year-old man. Arch Dermatol. 2001;137(4):495-500.
2. Fukuda H, Saito R. A case of Sister Mary Joseph’s nodule from prostatic cancer. J Dermatol. 2006;33(1):46-51.
3. Powell FC, Venencie PY, Winkelmann RK. Metastatic prostate carcinoma manifesting as penile nodules. Arch Dermatol.1984;120(12):1604-1606.
Aged Man with Disfigured Tip of Penis
Henry Schneiderman, MD
An 83-year-old man was examined on admission for end-of-life care due to profound dementia. His wife stated that his penis never changed in appearance, but believed that he always had concerns about it. To her knowledge, he never had trouble voiding. The patient was too impaired to discuss any topic coherently. His wife considered it unlikely that he would have disclosed any symptom of this type to her.
Physical examination. The patient was a markedly demented man. He did not show psychic or physical distress in his facial expression, body posture, or in the tone of his nonverbal vocalizations. He displayed no pressure ulcers. Upon examination, the patient had several scabbed areas on shins from bumping into things due to absent safety awareness and poor muscular control. He was breathing easily and quietly without any gurgling on secretions.

Discussion. Both phimosis and paraphimosis involve a prepuce and orifice that are too small for the glans. Phimosis, in which the skin is in the “forward position” overlying the glans, is well-tolerated unless the urine lacks proper egress or hygiene is compromised. In paraphimosis, the skin sits backward and acts as a constricting band, preventing venous and lymphatic return from the glans. This leads to edema of glans and shaft distal to the site of the constricting foreskin. As a result, the size disproportion is exacerbated and self-correction becomes impossible. In the extreme, without medical intervention, venous infarction of the distal penis may follow; this is why paraphimosis is a urological emergency, whereas phimosis is not.1,2
The embryology and life cycle of the foreskin are well-delineated.3 Some boys are born with a too-small preputial orifice; others lack the expected childhood reduction in adherence between layers of foreskin.3 Many boys and men develop adhesions and scarring due to infection, whether with Candida species, anaerobic bacteria, herpes viruses, sexually transmitted pathogens or unusual organisms.4-7 Phimosis can be caused by infection, however it also creates a closed space and thus predisposes to balanitis and posthitis.
A large subset of phimosis cases result from sterile inflammation, whether traumatic,8 from frostbite,9 iatrogenic, from radiotherapy,10 mechanical,11 or via the immunological condition balanitis xerotica obliterans, (a localized penile variant of lichen sclerosus et atrophicus).12 The newest inflammatory trigger to phimosis is bone marrow transplantation, perhaps via late scarring due to graft versus host disease.13
A relationship is reported between recent-onset phimosis in adults and diabetes mellitus.14 Several such patients had antecedent recurrent balanitis; another subset showed fissures of the foreskin: so the connection may be that diabetes predisposes to bacterial infection or mycosis of moist areas, and that the resultant inflammation and scarring creates phimosis.
The architecture of the penis predisposes to obstruction following injury: not only does the glans ordinarily vary in position relative to the foreskin, but also the entire penis has to accommodate substantial transient enlargement with each penile erection. It is not surprising that some patients’ symptoms first become noticeable upon sexual excitement.

Treatment. Very often, observation alone suffices as management of phimosis. Progression can warrant change to preempt worsening symptoms or cosmesis. Discomfiture, including psychological upset, calls for considering intervention. Many men dislike a phimotic appearance. Conversely, some Japanese men avoid circumcision for fear of its producing a 2-tone color change, to which Asian men seem particularly susceptible, that could embarrass them in a public bath.15
Recurrent symptomatic infections such as balanoposthitis require taking measures. So does any concern that cancer is lurking, invisible and thus undiagnosable, eg, with a lump under the foreskin or unexpected new phimosis in an older man. A mass would suggest late, advanced carcinoma or some less ominous condition such as Peyronie disease.
The most dramatic complication of phimosis is renal failure due to obstructive uropathy. One such case16 showed perfect recovery of renal function after relief of all obstruction and meticulous urological internal reconstruction. Patients waiting far too long to seek medical attention have the potential to wind up on lifetime dialysis.
At a minimum, obstruction must be considered in any man or boy with phimosis who reports that when he voids, the foreskin balloons before the urine exits to the toilet bowl. Be frank during examination, as embarrassment ensures that such information is unlikely to be volunteered after an open-ended question.
As with paraphimosis, circumcision sounds like a cure-all. But once again, a host of other measures have been devised and often achieve excellent results. Most involve repetitive retraction of the foreskin to break adhesions and to stretch the area17—capitalizing on the elasticity of skin in general and penile skin in particular—or the use of anti-inflammatory agents, or most often a combination of the two.18,19 The placebo arm of a study in which moisturizer was applied instead of the corticosteroid mometasone (drug information on mometasone), along with a program of parental stretching of boys’ phimotic foreskins, showed a 50% rate of resolution.
The pathologist’s histological examination of the prepuce would likely disclose some clinically unsuspected carcinomas, since occult cancers are sometimes found in hernia sacs and hemorrhoids. The frequency of incidental discovery of squamous cancer of the foreskin is low and lowest in boys and men whose circumcision is routine, whether performed for religious reasons or even for phimosis.20,21
Surprisingly, many foreskins from men with highly symptomatic phimosis show no scarring or inflammation at all, 20,21 re-emphasizing that some phimoses result purely from disproportion between size of glans/distal shaft and preputial orifice.
Discovery on histopathology of the inflammatory condition balanitis xerotica obliterans provides useful assistance by identifying a subgroup most at risk for subsequent meatal stenosis. Many such cases have already been recognized preoperatively by a urologist.
REFERENCES:
1. Schneiderman H. Paraphimosis in a man with a urethral catheter: the mimics of paraphimosis; and its many remedies. Consultant. 2004;44:275-281.
2. Choe JM. Paraphimosis: current treatment options. Am Fam Physician. 2000;62(12):2623-2626, 2628.
3. Lawless MR. The foreskin. Pediatr Rev. 2006;27(12):477-478.
4. Fox E. Phimosis. Practitioner. 1997;241(1578):534.
5. Tokgoz H. Preputial bacterial flora and its relation with phimosis. Urol Int. 2006;76(2):192.
6. White C, Sparks RA. Prepucial occlusion and circumcision after genital herpes infection. Int J STD AIDS. 1991;2(3):209-210.
7. Ariyanayagam-Baksh SM, Baksh FK, Cartun RW, Sieber PR. Histoplasma phimosis: an uncommon presentation of a not uncommon pathogen. Am J Dermatopathol. 2007;29(3):300-302.
8. Yip A, Ng SK, Wong WC, et al. Injury to the prepuce. Br J Urol. 1989;63(5):535-538.
9. Myhre U, Goode PN, Miller IA. Jogger’s phimosis. Br J Urol. 1989;63(5):549.
10. Featherstone JM, Aldridge A, Gudgeon AM. Radiotherapy for rectal carcinoma: an unusual cause of foreskin phimosis. Int Urol Nephrol. 2006;38(3-4):603-605.
11. Yuasa T, Kageyama S, Yoshiki T, Okada Y. Preputial calculi: a case report. Hinyokika Kiyo. 2001;47(7):513-515.
12. Neuhaus IM, Skidmore RA. Balanitis xerotica obliterans and its differential diagnosis. J Am Board Fam Pract. 1999;12(6):473-476.
13. Suzuki D, Kobayashi R, Kaneda M, et al. Severe phimosis as a notable sequela of allogeneic stem cell transplantation in boys. Bone Marrow Transplant. 2007;40(4):335-338.
14. Chopra R, Fisher RD, Fencl R. Phimosis and diabetes mellitus. J Urol. 1982;127(6):1101-1102.
15. Ohjimi H, Ogata K, Ohjimi T. A new method for the relief of adult phimosis. J Urol. 1995;153(5):1607-1609.
16. Rosenberg JW. Phimosis: a cause of renal failure. J Med Soc N J. 1983;80(10):845-846.
17. Dunn HP. Non-surgical management of phimosis. Aust N Z J Surg. 1989;59(12):963.
18. Pileggi F de O, Vicente YA. Phimotic ring topical corticoid cream (0.1% mometasone furoate) treatment in children. J Pediatr Surg. 2007;42(10):1749-1752.
19. Zampieri N, Corroppolo M, Camoglio FS, et al. Phimosis: stretching methods with or without application of topical steroids? J Pediatr. 2005;147(5):705-706.
20. Clemmensen OJ, Krogh J, Petri M. The histologic spectrum of prepuces from patients with phimosis. Am J Dermatopathol. 1988;10(2):104-108.
21. Pearce I, Payne SR. Do men having routine circumcision need histological confirmation of the cause of their phimosis or postoperative follow-up? Ann R Coll Surg Engl. 2002;84(5):325-327.