
A Collection of Hernias and Hernia-Associated Syndromes
Grynfeltt-Lesshaft Hernia
Lauren NG, MD, MPH, and Adam Possner, MD
A 52-year-old man presented to general internal medicine clinic with a 3-day history of stabbing left flank pain. He denied any fever, chills, dysuria, hematuria, nausea, vomiting, diarrhea, or constipation. Physical examination was significant for left flank tenderness.

Laboratory tests. A complete blood cell count, urinalysis, and basic metabolic panel, were all normal. An abdominal CT scan was then obtained, which revealed a 2.9 cm left lumbar hernia (arrow) through the superior triangle, known as a Grynfeltt-Lesshaft hernia.
Discussion. Lumbar hernias represent only about 2% of abdominal hernias. Predisposing factors include trauma, older age, obesity, extreme thinness or intense slimming, muscular atrophy, chronic bronchitis, and wound infection. The patient lacked these risk factors, but he did have a history of 2 bilateral inguinal hernia repairs, the most recent being 3 years ago.
Treatment. Grynfeltt-Lesshaft hernia treatment is always surgical.
Plummer-Vinson Syndrome
Mayada Issa, MD, Linda Green, MD, Jalil Ahari, MD, and Kalai Ayyanar, MD
A 44-year-old black woman presented to the emergency department with constipation of 4 days duration. She also complained of a sticking sensation in her throat over the past year and dysphagia to solids but not liquids. Over the past 2 years, she had an unintentional 40 lb weight loss, which she attributed to decreased appetite.
Two months earlier, the patient began to have shortness of breath on exertion; she had to rest after walking a few blocks and became dizzy when she rose quickly from a sitting position. She denied chest pain, orthopnea, and paroxysmal nocturnal dyspnea. Her menstrual history was significant for menorrhagia of 1 year duration.
Laboratory tests. The patient had pale conjunctivae, bilateral angular cheilitis, glossitis, and bilateral spoon-shaped nails (koilonychia). The white blood cell count was 7300/µL, hemoglobin level was 5.7 g/dL, platelet count at 555,000/µL, mean corpuscular volume at 55 fL, red blood cell distribution width at 22%, and ferritin at 6 ng/mL.

A pelvic ultrasonogram showed an enlarged uterus and multiple fibroids; the largest lesion was 5 cm. An upper GI barium study disclosed a cervical web on the anterior part of the esophagus. Upper endoscopy revealed thickening of the esophageal mucosa and a web, which was ruptured with the scope.
The authors diagnosed Plummer-Vinson syndrome (PVS) based on the following findings: history of painless dysphagia and the finding of an esophageal web; presence of glossitis, angular cheilitis, and koilonychias; and iron deficiency anemia caused by the long-standing menorrhagia secondary to fibroids.
PVS occurs most frequently in women age 30 to 70 years.1

Discussion. The syndrome is characterized by a triad of dysphagia, an esophageal web, and iron deficiency anemia.2 It has been associated with other causes of iron deficiency, such as celiac disease3 and a large diaphragmatic hernia that causes chronic blood loss.1
Iron repletion often ameliorates symptoms; however, some patients may require esophageal dilatation or bougienage.1,4 Since PVS is associated with an increased incidence of postcricoid carcinoma, patients with the syndrome require yearly endoscopic surveillance.4,5
Outcome of the case. This patient was transfused with 2 units of packed red blood cells followed by intravenous iron therapy. Her dysphagia and constipation resolved within a few days, and she was discharged. She was advised to take an oral iron supplement daily and to follow-up with her gynecologist. ■
References:
1. Maleki D, Cameron AJ. Plummer-Vinson syndrome associated with chronic blood loss anemia and large diaphragmatic hernia. Am J Gastroenterol. 2002;97(1):190-193.
2. Lopez Rodriguez MJ, Robledo Andres P, Amarilla Jimenez A, et al. Sideropenic dysphagia in an adolescent. J Pediatr Gastroenterol Nutr. 2002;
34(1):87-90.
3. Dickey W, McConnell B. Celiac disease presenting as the Paterson-Brown Kelly (Plummer-Vinson) syndrome. Am J Gastroenterol. 1999;94(2):
527-529.
4. Hoffman RM, Jaffe PE. Plummer-Vinson syndrome. A case report and literature review. Arch Intern Med. 1995;155(18):2008-2011.
5. Godino J, Wong PW. A triad of troubling findings. Plummer-Vinson syndrome. Postgrad Med. 2000;108(2):109-110.
Paraesophageal Hernia
Virendra Parikh, MD
A 79-year-old man presented with postprandial fullness and epigastric discomfort of 2 years duration. He also experienced regurgitation and substernal pain after eating that was relieved by belching. He has a history of hypertension and gout. The patient’s vital signs were normal on physical examination.
Laboratory tests. A chest radiograph showed haziness with an airfluid level in the left costophrenic angle, close to the cardiac apex (Figure 1). Results of an upper GI barium swallow study revealed a paraesophageal hernia (Figure 2). A portion of the stomach was seen in the intrathoracic position. All laboratory test results were within normal limits.

Discussion. Paraesophageal hernias are more common with advanced age. Most are asymptomatic when discovered early. Symptoms of pain, fullness, and eructation are intermittent and episodic. Chronic anemia from gastritis is common. Substernal pain may be confused with cardiac angina; a nitroglycerin trial can rule out this entity.
Treatment. All patients with this type of hernia are at risk for obstruction and strangulation of the herniated stomach. Paraesophageal hernias require surgical repair. This can be done by laparoscopic method, laparotomy, or thoracotomy. The likelihood of recurrence is small (less than 5%). This patient recovered well after surgery.
Gastric Volvulus
Steven R. Bruhl, MD, MS, Hollis W. Merrick, MD, and Basil E. Akpunonu, MD
An 88-year-old woman was brought to the emergency department after she choked on a piece of meat. She had dysphagia of many years’ duration and progressive weight loss over the past 5 years.
Physical examination. Physical findings were unremarkable. Radiographs of the chest and abdomen showed a gastric bubble in the left lower thoracic cavity (Figure A). A barium swallow showed the stomach within the thorax (Figure B).
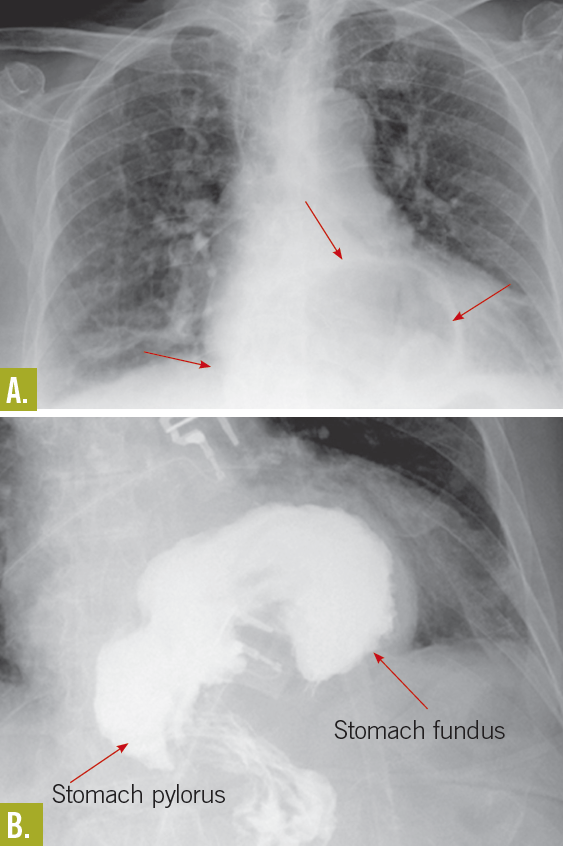
Discussion. An organoaxial volvulus is a type of gastric volvulus—a rare but serious disorder—in which the stomach rotates superiorly along its long axis. The rotation must be ≥180° and is usually associated with diaphragmatic defects. The rotation causes the greater curvature of the stomach to be superior to the lesser curvature; as a result, the stomach appears upside down.
About 60% of cases are organoaxial and 30% are mesenteroaxial, in which the stomach rotates along its short axis. This less common form is usually associated with ligamentous laxity. The remaining 10% of cases are a mixed type.1 The disorder can be further classified as subdiaphragmatic, or primary (33% of cases), in which the cause is usually congenital, or as supradiaphragmatic, or secondary (67% of cases), which is generally caused by trauma or associated with diaphragmatic defects.2
Typical symptoms of a long-term gastric volvulus include dysphagia and intermittent abdominal pain that is often brought on by large meals. Traumatic presentations represent a surgical emergency and often include severe epigastric pain, inability to vomit, and difficult nasogastric tube insertion—known as Borchardt triad.
An undetected gastric volvulus can develop into a closed-loop obstruction that may lead to incarceration, strangulation, ischemia, or gastric perforation. Mortality varies depending on the cause and severity of the disorder, but it is reportedly about 42% to 56% in acute cases and 10% to 13% in chronic cases.3
Outcome of the case. This patient underwent corrective Nissen fundoplication, hiatal hernia repair, and gastropexy. She recovered without complication.
References:
1. Godshall D, Mossallam U, Rosenbaum R. Gastric volvulus: case report and review of the literature. J Emerg Med. 1999;17(5):837-840.
2. Cozart JC, Clouse RE. Gastric volvulus as a cause of intermittent dysphasia. Dig Dis Sci. 1998;43(5):1057-1060.
3. Green J, Stein M. Gastric volvulus imaging. Medscape emedicine. www.emedicine.com/radio/topic296.htm. Accessed March 16, 2011.
Diaphragmatic Hernia
Mark Macelwee, MD, and Zachary Hartsell, MPAS
A 67-year-old man presented to the emergency department with flank pain of 4 days duration. A right obstructing ureteric calculus, acute renal failure, and “perinephric reaction” were diagnosed. Preoperative medical consultation revealed a history of a motor vehicle accident with diaphragmatic eventration, probable vocal cord paralysis, and dysphonia. The patient had no other significant past medical history. He had undergone recent outpatient stress echocardiography, which was negative, and he reported that he was able to perform vigorous daily aerobic exercise without difficulty.
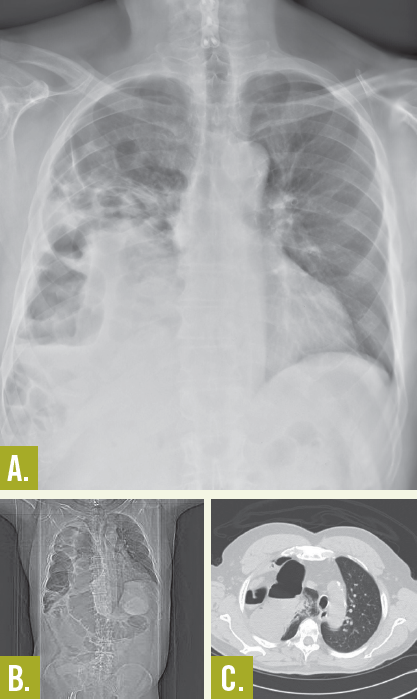
Laboratory tests. A preoperative ECG was unremarkable. The preoperative chest radiograph (Figure A) demonstrated abnormalities consisting of pulmonary encroachment by expansion of a diaphragmatic hernia. The patient was medically stable for surgery, and perioperative airway management recommendations were conveyed that advised the avoidance of bag mask ventilation and use of a laryngeal mask. The patient was taken to the operating room for a ureteral stone removal under general anesthesia. Multiple attempts at endotracheal intubation were unsuccessful, and ultimately a #5 laryngeal mask airway (LMA) was placed. The patient tolerated cystoscopy with stone extraction and was discharged home later in the day.
He returned to the emergency department with complaints of worsening shortness of breath. A radiograph (Figure B) and CT scan (Figure C) demonstrated atelectasis of the right lung with opacified loops of bowel in the thorax. The patient was taken for emergent laparotomy, reduction, and repair of a diaphragmatic hernia.
Discussion. A paucity of literature in either the pediatric or adult disciplines exists regarding perioperative risk and management of diaphragmatic hernias. Extrapolation from neonatal practice with congenital hernias led to our recommendations to decompress the stomach and avoid bag mask ventilation or LMA.
Review of the literature did not identify randomized studies and only disclosed a few case reports with various anecdotal recommendations.1,2 One of the case reports involved a patient who had a diaphragmatic injury and underwent an elective lumbar laminectomy. The patient tolerated the procedure well, undergoing perioperative prophylactic GI decompression, endotracheal intubation, and positioning to allow the abdomen to be freely dependent.2
Literature suggests that traumatic diaphragmatic hernias are relatively common and occur in 5% to 10% of patients who are involved in motor vehicle accidents or who sustain penetrating trauma.
Recommendations include a low threshold for obtaining a preoperative chest radiograph based on risk assessment, history of chest trauma, or severe reflux symptoms. In addition, empiric nasogastric tube insertion, perioperative antacids, and avoidance of prolonged bag valve mask or LMA are strategies that may decrease postoperative pulmonary complications in patients with untreated diaphragmatic hernias.
Outcome of the case. The patient underwent intraoperative colonoscopy and cecostomy tube placement for bowel decompression. Postoperatively, the patient developed a deep venous thrombosis that required anticoagulation and a prolonged ileus that required total parenteral nutrition. He was ultimately discharged on warfarin and wound care for his colostomy.
References:
1. Dietrich CL, Smith CE. Anaesthesia for Caesarean delivery in a patient with an undiagnosed traumatic diaphragmatic hernia. Anesthesiology. 2001;4:
1028-1031.
2. Katz RI, Belenker SL, Poppers PJ. Intraoperative management of a patient with a chronic, previously undiagnosed traumatic diaphragmatic hernia.
J Clin Anesth. 1998;10:506-509.