
Adrenocortical Insufficiency: An Overview of Evaluation and Management
Author:
Kim A. Carmichael, MD
Citation:
Carmichael KA. Adrenocortical insufficiency: an overview of evaluation and management. Consultant. 2017;57(5, Suppl.):S4-S6.
Adrenocortical insufficiency (AI) is an uncommon medical disorder that may be either primary, with loss of adrenal gland function and occurring in approximately 93 to 140 persons per million,1,2 or secondary, due to impaired stimulation and occurring in approximately 150 to 280 persons per million.1 Recognition and appropriate management of AI is important, since insufficient cortisol levels can result in severe medical illness and crisis such as hypotension, hypoglycemia, and even death.
Clinical Manifestations
AI may present acutely, such as in the intensive care unit (ICU), or may be insidious with nonspecific symptoms. AI is rare, but its seriousness warrants a high index of suspicion.3
In the ICU, AI may present with hypotensive shock, abdominal pain, agitation, confusion, lethargy, fever, or hypoglycemia.3,4 In other settings, the presentation may be gradual in onset, with general fatigue, weakness, orthostatic hypotension, anorexia, anxiety, or hypoglycemia. In pregnancy, women with AI may have unexplained fatigue, nausea, and hypotension.3 Primary AI also may be associated with salt craving due to mineralocorticoid deficiency, particularly with hyperkalemia and hyponatremia.1,2,4,5
Etiology
Primary AI is a result of autoimmune disease in 80% to 90% of patients in North America and Europe,1,2,4,5 with 40% occurring in polyglandular endocrine syndromes such as concomitant hypothyroidism, Graves disease, vitiligo, alopecia, celiac disease, or pernicious anemia. In developing populations, AI may be related to tuberculosis or other granulomatous disorders. Other potential causes include hereditary disorders such as congenital adrenal hyperplasia, infiltrative diseases, adrenalectomy, adrenal hemorrhage (often with associated coagulation disorders), insensitivity syndromes, genetic metabolic disorders, or the use of certain medications.3
Primary AI results in deficiencies of both glucocorticoids and mineralocorticoids, thereby increasing the risks of hypotension, dehydration, and electrolyte disorders.
Secondary AI is most commonly iatrogenic, related to chronic glucocorticoid therapy.6 Otherwise, secondary AI may be associated with infiltrative or traumatic pituitary or hypothalamic disorders, subarachnoid hemorrhage, or the use of a number of medications. Megestrol acetate is particularly associated with AI, more commonly among children.7 Secondary AI, in contrast with primary AI, does not result in mineralocorticoid deficiency and ordinarily is not associated with electrolyte disturbances.
Physical Examination and Evaluation
AI often is associated with minimal physical manifestations, but hyperpigmentation of skin and mucosal surfaces may occur in primary AI.1,2 Patients may have orthostatic hypotension, particularly in the setting of mineralocorticoid deficiency. Axillary and/or pubic hair may be sparse or absent, particularly in women.
In noncritical settings, early-morning cortisol levels may confirm AI if they are less than 3 µg/dL or rule out AI if they are 18 µg/dL or greater.1 In the case of intermediate corstisol levels, a cosyntropin stimulation test may be useful.1,2,4,8 When cosyntropin is injected, elevation of the serum cortisol level to above 15 µg/dL rules out primary AI and above 18 µg/dL rules out secondary AI. The 250-µg dose cosyntropin test is 97% sensitive for primary AI and 57% sensitive for secondary AI.8
When AI is suspected in patients in the ICU, they should immediately receive stress-dose corticosteroids if there is hemodynamic instability or acute respiratory distress syndrome.3,9 The results of an adrenocorticotropic hormone (ACTH, cosyntropin [synthetic]) stimulation test or other laboratory tests should not be used as the basis for therapy.4,9 The preferred medications are intravenous hydrocortisone, 100 mg immediately then 200 mg/d as maintenance, or prednisolone.3 Depending on the clinical presentation, a baseline random cortisol level of less than 10 µg/dL suggests that AI is likely, and a cosyntropin-stimulated cortisol level of greater than 43 µg/dL suggests that AI is highly unlikely.10
Plasma ACTH levels may distinguish primary AI (elevated) from secondary (suppressed) AI,1-5 and low plasma aldosterone levels with high renin may be seen in primary AI.1,3 Insulin tolerance testing and metyrapone testing should be limited to specialty centers with experience in using these techniques.
Other potentially abnormal blood test results associated with AI include low sodium and glucose levels, high potassium and calcium levels, and altered free thyroxine and thyrotropin levels (in the setting of either concomitant hypothyroidism or concomitant Graves disease).
The Endocrine Society’s clinical practice guidelines3 include the recommendation of testing 17-hydroxyprogesterone and 21-hydroxylase antibodies to guide the evaluation of the etiology of primary AI. These test results can then indicate the pathway for further evaluation.
Adrenal imaging is not needed with autoimmune AI or adrenomyeloneuropathy,2 but it may be useful when infectious or infiltrative diseases are suspected. Pituitary/hypothalamic imaging may be useful in secondary AI.1,2,5
Management
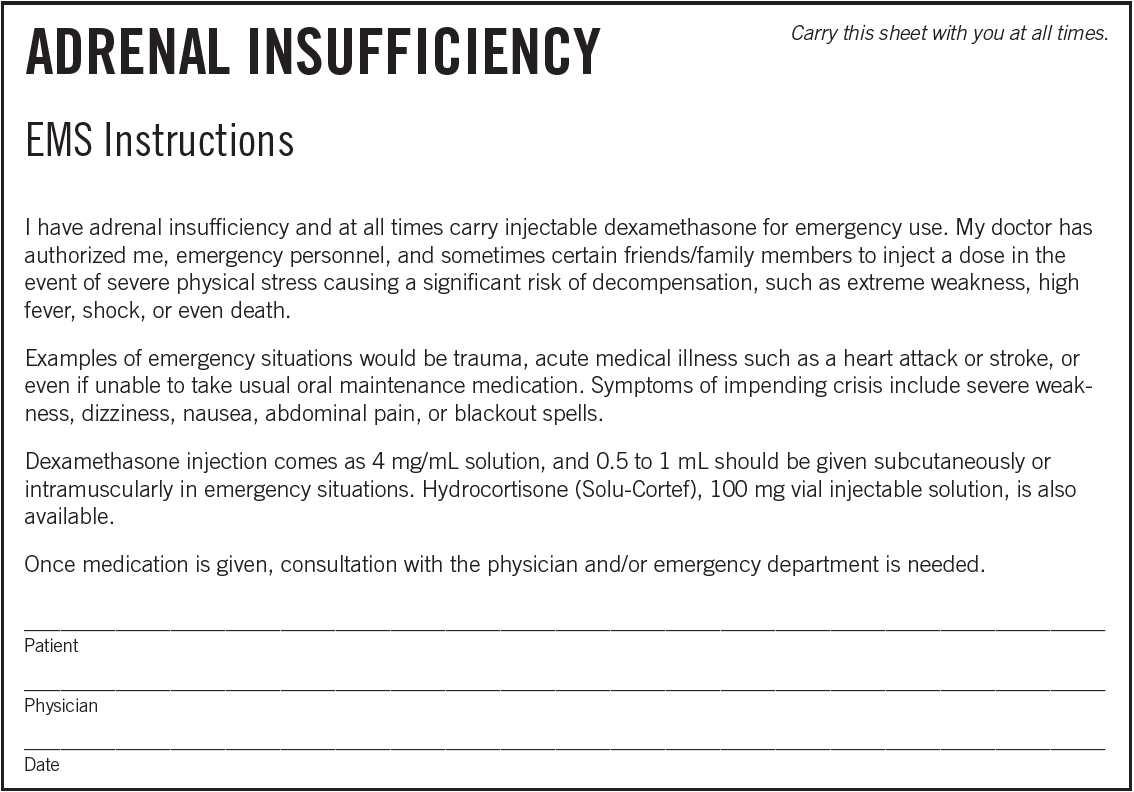
Persons with AI should carry medical alert identification (Sidebar) and an emergency injectable glucocorticoid such as dexamethasone or hydrocortisone. Patients should be educated on the symptoms of low or excessive cortisol levels and to double or triple their baseline glucocorticoid medication in the setting of significant physiologic stress.
Dosing of glucocorticoids needs to be individualized, most commonly using hydrocortisone, 15 to 25 mg daily, or cortisone acetate, 20 to 35 mg daily in 2 or 3 divided doses, with the highest dose in the early morning.3 Alternatively, prednisolone, 3 to 5 mg daily, or prednisone, 4 to 7 mg daily, may be used in 2 or 3 divided doses. Fludrocortisone, 0.05 to 3.0 mg daily, also may be needed for the treatment of persons with primary AI,2,5 and patients should not restrict their salt intake.3
There currently is no evidence to either support or reject the use of supplemental perioperative corticosteroids for adults on maintenance therapy, but clinical practice guidelines support their use, including at the time of delivery (with hydrocortisone preferred).3
Dehydroepiandrosterone may be tried for women with low energy and depressive symptoms despite optimal glucocorticoid therapy, with periodic monitoring of blood levels.3 This therapy should be discontinued after 6 months if no symptom improvement has occurred.
Follow-up management of AI includes monitoring for inadequate glucocorticoid replacement therapy in patients with fatigue, orthostatic hypotension, and weight loss, or for excessive glucocorticoid replacement therapy in patients with weight gain, striae and excessive bruising, hypertension, hyperglycemia, and osteopenia. Monitoring with glucocorticoid and ACTH levels is not recommended.3 In patients with autoimmune AI, periodic surveillance for other autoimmune disorders such as thyroid disease and vitamin B12 deficiency should be performed.3
AI is a serious medical condition that may have an insidious onset and minimal external clinical clues. It should be suspected in the setting of unexplained fatigue, hypotension, and hypoglycemia. This is particularly important during acute illness in the setting of known risk factors. Early recognition and management of AI are important to improve patient well-being and prevent serious hemodynamic and metabolic complications.
Kim A. Carmichael, MD, is an associate professor of medicine in the Department of Medicine, Division of Endocrinology, Metabolism and Lipid Research, at Washington University School of Medicine in St Louis, Missouri.
REFERENCES:
- Wallace I, Cunningham S, Lindsay J. The diagnosis and investigation of adrenal insufficiency in adults. Ann Clin Biochem. 2009;46(pt 5):351-367.
- Nieman LK, Chanco Turner ML. Addison’s disease. Clin Dermatol. 2006;24(4):276-280.
- Bornstein SR, Allolio B, Arlt W, et al. Diagnosis and treatment of primary adrenal insufficiency: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2016;101(2):364-389.
- Bouillon R. Acute adrenal insufficiency. Endocrinol Metab Clin North Am. 2006;35(4):767-775.
- Arlt W, Allolio B. Adrenal insufficiency. Lancet. 2003;361(9372):1881-1893.
- Bornstein SR. Predisposing factors for adrenal insufficiency. N Engl J Med. 2009;360(22):2328-2339.
- Orme LM, Bond JD, Humphrey MS, et al. Megestrol acetate in pediatric oncology patients may lead to severe, symptomatic adrenal suppression. Cancer. 2003;98(2):397-405.
- Dorin RI, Qualls CR, Crapo LM. Diagnosis of adrenal insufficiency. Ann Intern Med. 2003;139(3):194-204.
- Marik PE, Pastores SM, Annane D, et al. Recommendations for the diagnosis and management of corticosteroid insufficiency in critically ill adult patients: consensus statements from an international task force by the American College of Critical Care Medicine. Crit Care Med. 2008;36(6):1937-1949.
- Annane D, Maxime V, Ibrahim F, Alvarez JC, Abe E, Boudou P. Diagnosis of adrenal insufficiency in severe sepsis and septic shock. Am J Res Crit Care Med. 2006;174(12):1319-1326.