
Peer Reviewed
Mucoepidermoid Carcinoma Causing Localized Recurrent Pneumonia in a 7-Year-Old Boy
AUTHORS:
Aisha Baig, MD
Assistant Professor, Department of Pediatrics, Pulmonary Division, Robert Wood Johnson University Hospital, New Brunswick, New Jersey
Saurabh Gupta, MD
Assistant Professor of Radiology and Section Chief of Pediatric Radiology Section, Diagnostic Division, Upstate University Hospital, Syracuse, New York
CITATION:
Baig A, Gupta S. Mucoepidermoid carcinoma causing localized recurrent pneumonia in a 7-year-old boy [published online February 6, 2020]. Pulmonology Consultant.
A 7-year-old previously healthy and active boy without comorbidities presented to the pulmonary clinic with a 6-month history of dry cough, recurrent left lower lobe pneumonia, and limited physical activity. He had been on several rounds of oral antibiotics, oral and inhaled corticosteroids, and bronchodilator therapy with no significant improvement in his respiratory symptoms.
Physical examination revealed normal respiratory rate and oxygen saturation. On lung auscultation, breath sounds were absent on the left lower lung. Breath sounds on the right lung were normal. The remainder of physical examination findings were unremarkable.
A chest radiograph revealed left upper lobe atelectasis and left lower lobe hyperinflation (Figure 1) with the ball-valve effect suggestive of air trapping.

Figure 1. Posteroanterior view of the chest showing atelectasis of the left upper lobe and hyperinflated left lower lobe with mediastinal shift.
A computed tomography (CT) scan with contrast showed a nodular endobronchial lesion in the left mainstem bronchus with left upper lobe and lingular atelectasis and a hyperinflated left lower lobe. An azygos fissure was noted in the right lung (Figure 2).
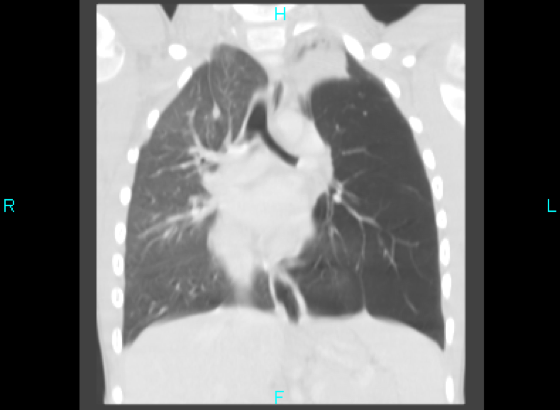
Figure 2. Coronal contrast CT image showing a nodular endobronchial lesion in the left mainstem bronchus with left upper lobe and lingular atelectasis and a hyperinflated left lower lobe. An azygos fissure was noted in the right lung.
Flexible bronchoscopy and rigid bronchoscopy findings showed a polypoid, tan-colored mass in the distal left mainstem bronchus, with almost complete occlusion of the bronchus (Figure 3).

Figure 3. An obstructive endobronchial lesion at the distal entry of the left mainstem bronchus.
DISCUSSION
The differential diagnoses of endobronchial lesion include aspiration of foreign objects, respiratory tract papillomatosis, inflammatory myofibroblastic tumor, adenoid cystic carcinoma, neuroendocrine tumor, bronchial carcinoid tumor, mucoepidermoid carcinoma, and endobronchial hamartoma.1-3
Our patient was started on antibiotics to treat any underlying infectious processes beyond the mass and was transferred to an advanced pediatric subspecialty center. There, results of an interventional bronchoscopy confirmed similar findings. Histology test results of the initial forceps biopsy of the lesion revealed features consistent with salivary gland neoplasm: epithelial cells positive for cytokeratin AE1/AE3 by immunochemical stain and negative for neuroendocrine markers such as synaptophysin and CD56.
He then underwent surgical resection of the mass, histology test results of which showed hypocellular spindled stromal cells with a myxoid background. Further genetic processing with fluorescence in situ hybridization DNA analysis confirmed translocation of the mastermind like transcriptional coactivator 2 gene (MAML2), specific for mucoepidermoid carcinoma (MEC).
MEC accounts for 0.1% to 0.2% of primary lung tumors.1 It is defined by a combination of mucus-secreting squamous and intermediate cell types.1 The reported age range is wide, from 2 to 78 years, with both sexes affected equally.1,4-6
In the airway, MEC arises from the submucosal bronchial glands and primarily affects the main or lobar bronchi, but it can involve any segmental bronchi or peripheral lung,1,2,7 Most common symptoms of pulmonary MEC are due to large airway obstruction and include cough, bronchitis, hemoptysis, chest pain, postobstructive recurrent pneumonia, and pulmonary abscesses.1,3,6-9 Rare cases of pulmonary MEC can present as a pneumothorax.8
Diagnosis is often delayed due to the rarity of the condition, with some studies citing an average of 11 months.1,7,10
On chest radiographs, MEC presents as area of central airway mass with postobstructive pneumonia or peripheral atelectasis, and on CT as a smooth oval or lobulated airway mass obstructing the bronchus.1,2,5 On bronchoscopy, the tumor usually appears as a smooth, rounded, tan-colored mass with intact overlying mucosa.5,8,10
Several different chromosomal translocations have been identified in MEC tumors. The most common is t(11;19)(q21;p13), which creates a fusion gene, MECT1-MAML2 (MEC translocated-1-mastermind-like 2).1,8,11-13 The presence of MECT1-MAML2 is associated with lower clinical stage, low-grade tumor histopathology and a favorable prognosis,12-14 as was the case in our patient.
OUTCOME OF THE CASE
Based on the recommendations of the oncology and thoracic surgery team, the decision was made to excise the endobronchial lesion to increase disease-free survival. The patient successfully underwent complete surgical resection of the mass and reconstruction of the left mainstem bronchus. The mass was 1.1 cm in size, histologically classified as low grade, with no lymph node involvement, and the margins were free of the tumor.
At his 1-year follow-up visit in the pulmonary clinic, the patient remained completely symptom-free, with normal lung examination findings. He remains very physically active.
REFERENCES:
- Liu X, Adams AL. Mucoepidermoid carcinoma of the bronchus: a review. Arch Pathol Lab Med. 2007;131(9):1400-1404.
- Kim TS, Lee KS, Han J, et al. Mucoepidermoid carcinoma of the tracheobronchial tree: radiographic and CT findings in 12 patients. Radiology. 1999;212(3):643-648. doi:10.1148/radiology.213.r99se09643
- Qian X, Sun Z, Pan W, Ye Q, Tang J, Cao Z. Childhood bronchial mucoepidermoid tumors: a case report and literature review. Oncol Lett. 2013;6(5):1409-1412. doi:10.3892/ol.2011529
- Szymanski LJ, Molas-Torreblanca K, Bawab R, et al. Bronchial mucoepidermoid carcinoma with the classic MAML2 gene rearrangement in a 2-year-old boy. Pediatr Dev Pathol. 2018;21(5):480-485. doi:10.1177/1093526617707855
- Saoud M, Patil M, Dhillon SS, et al. Rare airway tumors: an update on current diagnostic and management strategies. J Thorac Dis. 2016;8(8):1922-1934. doi:10.21037/jtd.2016.07.40
- Horst M, Dekker M, Braak S. Mucoepidermoid carcinoma of the airways in a young adult male. J Radiol Case Rep. 2017;11(2):8-15. doi:10.3941/jrcr.v11i2.3061
- Vageriya NL, Shah RS, Prabhu S, Naphade D, Athawale HR. Intra bronchial mucoepidermoid carcinoma in an 8 year old girl: a case report of rare tumor with review of literature. J Pediatr Surg Case Rep. 2016;13:41-44. doi:10.1016/j.epsc.2016.0002
- Kose M, Bilgin M, Kontas O, Ozturk S, Doganay S, Ozdemir MA. A case of mucoepidermoid carcinoma of the bronchus presented with hydropneumothorax in a child. Pediatr Pulmonol. 2014;49(3):E86-E89. doi:10.1002/ppul.22938
- Firinci F, Ates O, Karaman O, et al. A 7-year-old girl with cough, fever, pneumonia. Pediatr Ann. 2011;40(3):124-127. doi:10.3928/00904481-20110217-04
- Giusti RJ, Flores RM. Mucoepidermoid carcinoma of the bronchus presenting with a negative chest x-ray and normal pulmonary function in two teenagers: two case reports and review of the literature. Pediatr Pulmonol. 2004;37(1):81-84. doi:1002/ppul.10390
- Tonon G, Gehlhaus KS, Yonescu R, Kaye FJ, Kirsch IR. Multiple reciprocal translocations in salivary gland mucoepidermoid carcinomas. Cancer Genet Cytogenet. 2004;152(1):15-22. doi:10.1016/j.cancergencyto.2003.10.007
- Martins C, Cavaco B, Tonon G, Kaye FJ, Soares J, Fonseca I. A study of MECT1-MAML2 in mucoepidermoid carcinoma and Warthin’s tumor of salivary glands. J Mol Diagn. 2004;6(3):205-210. doi:10.1016/S1525-1578(10)60511-9
- Omesh T, Gupta R, Saqi A, Burack J, Khaja M. A rare case of endobronchial mucoepidermoid carcinoma of the lung presenting as non-resolving pneumonia. Respir Med Case Rep. 2018;25:154-157. doi:10.1016/j.rmcr.2018.08.014
- Techavichit P, Hicks MJ, López-Terrada DH, et al. Mucoepidermoid carcinoma in children: a single institutional experience. Pediatr Blood Cancer. 2016;63(1):27-31. doi:10.1002/pbc.25681