
Man With an Intraocular Mass
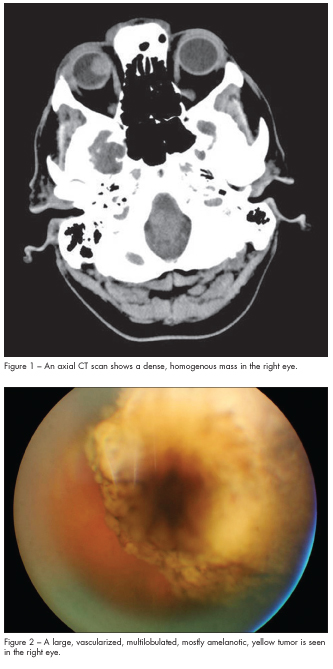 A 53-year-old man presents for evaluation of an intraocular mass in his right eye. One month earlier he had tripped over a space heater and hit his forehead on a countertop. At that time he was treated in an urgent care clinic for a laceration on his left forehead. Because he had a persistent chronic headache after his head trauma, he followed up with his family physician. The physician ordered a CT scan of the head, which revealed a large, dense, homogenous mass in the right eye (Figure 1).
A 53-year-old man presents for evaluation of an intraocular mass in his right eye. One month earlier he had tripped over a space heater and hit his forehead on a countertop. At that time he was treated in an urgent care clinic for a laceration on his left forehead. Because he had a persistent chronic headache after his head trauma, he followed up with his family physician. The physician ordered a CT scan of the head, which revealed a large, dense, homogenous mass in the right eye (Figure 1).
The patient has hypertension for which he is taking lisinopril. He has been a smoker for 27 years. He has had no recent weight loss or anorexia. This is his first dilated eye examination. He denies any vision changes, flashing lights, or new floaters, and he does not have any eye pain. He does have a headache located on top of his head and in the left forehead area; it occurs daily and is worse toward the end of the day.
The patient’s corrected visual acuity is 20/20 in each eye. Results of his pupil and motility examinations are unremarkable. His intraocular pressures are normal and symmetrical between the two eyes. A visual field examination reveals an infratemporal step in the right eye. The left eye has no defects.
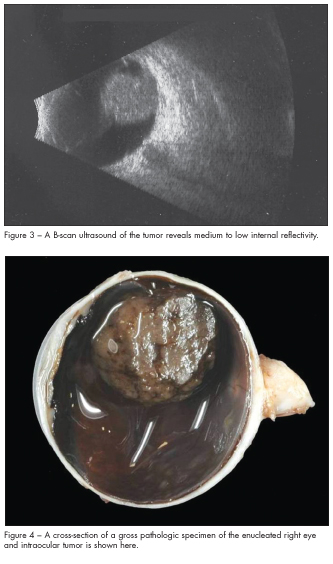
A slit lamp evaluation is unremarkable as is a dilated fundus examination of the left eye. Funduscopic examination of the right eye reveals pigmented cells in the vitreous and a large, vascularized, multilobulated yellowish tumor involving the superonasal quadrant of the retina (Figure 2). A B-scan ultrasound shows a well-circumscribed homogenous tumor measuring 18 mm 3 15 mm (basal dimensions) and a height of 12 mm (Figure 3).
The patient is seen by an ocular oncologist. His medical evaluation, which includes positron emission tomography (PET) testing, is negative for metastases.
Because of the large size of the tumor and the high probability that it is a malignancy, the patient undergoes an enucleation of the right eye (Figure 4). Histopathology findings confirm a spindle cell choroidal melanoma (Figures 5 and 6).
Testing for monosomy 3 chromosomal abnormality is negative. The patient continues to be monitored annually with liver function tests and PET scans. He is also now wearing safety glasses to protect his left eye.
CHOROIDAL MELANOMA: AN OVERVIEW
Epidemiology. Uveal melanoma is the most common primary malignant intraocular tumor in adults.1-3 Ninety percent of uveal melanomas develop in the choroid.1 In the United States, uveal melanoma is diagnosed in 6 or 7 persons per million each year.1-3 The incidence rises with increasing age: 65% of patients with melanoma are over the age of 50 years.3
Risk factors for choroidal melanoma include Caucasian race, light iris color, freckling as a child, nevi on the upper arms, dysplastic nevus syndrome, atypical ocular nevi, and ocular and oculodermal melanocytosis.4-6 Males are affected more often than females.4
Clinical presentation. Patients are often asymptomatic unless part of the tumor impinges on the visual axis or causes macular edema.7 Findings include a brown or golden mass, which may have an orange pigment (lipofuscin) on its surface. If the tumor breaks through Bruch’s membrane, it will have a dome or mushroom shape.7,8 Subretinal fluid may accumulate in association with a choroidal melanoma, producing vision loss.8
Classification. A choroidal melanoma is often classified by its size and histology. Melanoma can be classified by size according to the Collaborative Ocular Melanoma Study (COMS).3,9 A small melanoma has a largest basal diameter of more than 5 mm and apical height from 1 to 2.5 mm. A melanoma is classified as medium if the largest basal diameter is equal to or less than 16 mm or its apical height is 2.5 to 10 mm. If the largest basal diameter is greater than 16 mm or the apical height is greater than 10 mm, the tumor is classified as large.
 Histologically, choroidal melanomas are composed of spindle cells, epitheliod cells, or a mixed combination of the two kinds of cells.7 In the COMS study of enucleated eyes that had choroidal melanomas, 86% were found to be mixed cell type, 9% spindle cell, and 5% epitheliod cell type.10
Histologically, choroidal melanomas are composed of spindle cells, epitheliod cells, or a mixed combination of the two kinds of cells.7 In the COMS study of enucleated eyes that had choroidal melanomas, 86% were found to be mixed cell type, 9% spindle cell, and 5% epitheliod cell type.10
Evaluation. A dilated fundus examination is often sufficient for the diagnosis of the vast majority of ocular melanomas. Other special investigations can be used in questionable cases or in helping to confirm the diagnosis. Fluorescein and indocyanine green retinal angiography can show whether the tumor has vascular features.11 Ultrasound is useful in detecting tumors when the ocular media is opaque and when there is extraocular extension, and it is helpful in measuring tumor dimensions.7,11 On a CT scan, a melanoma will appear hyperdense; on an MRI scan, it will appear hyperintense on T-1 imaging and hypointense on T-2 imaging.7,11
Uveal melanomas tend to metastasize to the liver, lung, central nervous system, bone, and skin.12 A baseline evaluation for metastases should include a complete physical examination, complete blood cell count, serum liver enzyme panel, chest radiography, and liver imaging.13 PET has been found to be beneficial as a baseline evaluation for metastatic disease.14
Treatment. For many years enucleation was the only treatment available for choroidal melanoma. It is still the treatment of choice for large tumors, for optic disc invasion, and if there is irreversible loss of useful vision. For small or medium size tumors, the choice of management depends on the characteristics of the individual tumor. Transpupillary thermotherapy (TTT) is a technique that uses a diode laser to deliver infrared radiation to the tumor, which causes tumor cell necrosis.
It works best for pigmented tumors.15 Radiotherapy such as plaque brachytherapy using iodine-125, ruthenium-106, or other isotopes is used for smaller tumors and can be used in combination with TTT in a technique called sandwich therapy.8
Prognosis. The long-term status of patients after treatment for choroidal melanoma has been reported by the COMS investigators.16 Overall, at 5 years, 25% of patients had metastatic melanoma and 34% had the diagnosis at 10 years. When patients were separated by tumor size, 43% of those with a large tumor and 23% with a medium size tumor had metastasis at 5 years. Another study that investigated a longer-term prognosis found that by 35 years, 52% of its participants were dead because of uveal melanoma.17 Typically, a patient lives only 6 to 12 months beyond the diagnosis of metastatic disease.16
Loss of chromosome 3 and gains in chromosome 8 are associated with a poor prognosis. Gains in the short arm of chromosome 6 carry a favorable prognosis.7

1. Economou MA. Introduction: uveal melanoma. Acta Ophthalmol. 2008;83:7-19.
2. Bell DJ, Wilson MW. Choroidal melanoma: natural history and management options. Cancer Control. 2004;11:296-303.
3. Margo C. The Collaborative Ocular Melanoma Study: an overview. Cancer Control. 2004;11:304-309.
4. Margo CE, Mulla Z, Billiris K. Incidence of surgically treated uveal melanoma by race and ethnicity. Ophthalmology. 1998;105:1087-1090.
5. Stang A, Ahrens W, Anastassiou G, Jockel K. Phenotypical characteristics, lifestyle, social class and uveal melanoma. Ophthalmology Epidemiology. 2003;10:293-302.
6. Schmidt-Pokrzywniak A, Jockel K, Bornfeld N, et al. Positive interaction between light iris color and ultraviolet radiation in relation to the risk of uveal melanoma.Ophthalmology. 2009;116:340-348.
7. Kanski JJ, Bowling B. Clinical Ophthalmology: A Systematic Approach. 7th ed. Edinburgh: Elsevier Saunders; 2011:496-504.
8. Baumal CR, Baker BJ. Pigmented lesions of the fundus: discrete small to medium size. In: Steidl SM, Hartnett ME, eds. Clinical Pathways in Vitreoretinal Disease.New York: Thieme; 2003:99-113.
9. Singh AD, Kivela T. The Collaborative Ocular Melanoma Study. Ophthalmol Clin N Am. 2005;18:129-142.
10. Collaborative Ocular Melanoma Study Group. Histopathologic characteristics of uveal melanomas in eyes enucleated from the Collaborative Ocular Melanoma Study COMS Report No. 6. Am J Ophthalmol. 1998;125:745-766.
11. Bakri S, Sculley L, Singh A. Imaging techniques of uveal melanoma. International Ophthalmol Clin. 2006;46:1-13.
12. Shanmugam MP, Murthy PR, Murthy KR. Ocular oncology. In: Saxena S, ed. Clinical Ophthalmology: Medical & Surgical Approach. 2nd ed.
New Delhi: Jaypee Brothers Medical Publishers; 2011:647-669.
13. Diener-West M, Reynolds S, Agugliaro D, et al. Screening for metastasis for choroidal melanoma: The Collaborative Ocular Melanoma Study Group Report 23. J Clin Oncology. 2004;18:2438-2444.
14. Faia LJ, Pulido JS, Donaldson MJ, et al. The relationship between combined positron emission tomography/computed tomography and clinical and light microscopic findings in choroidal melanoma. Retina, J Retina Vit Disease. 2008;28:763-769.
15. Aaberg TM, Bergstrom CS, Hickner ZJ, Lynn MJ. Long-term results of primary transpupillary thermal therapy for the treatment of choroidal malignant melanoma.Br J Ophthalmol. 2008;92:741-746.
16. Collaborative Ocular Melanoma Study Group. Development of metastatic disease after enrollment in the COMS trials for treatment of choroidal melanoma. Arch Ophthalmol. 2005;123:1639-1643.
17. Kujala E, Makitie R, Kivela T. Very long-term prognosis of patients with malignant uveal melanoma. Invest Ophthalmol Vis Sci. 2003;44:4651-4659.