
Peer Reviewed
Gastric Signet-Ring Cell Carcinoma With Bladder Metastasis
Authors:
Michael Krzyzak, MD; Richard M. Felix, MD; Jocelyn Villanueva, MD; and Stephen Mulrooney, MD
Staten Island University Hospital, Staten Island, New York
Citation:
Krzyzak M, Felix RM, Villanueva J, Mulrooney S. Gastric signet-ring cell carcinoma with bladder metastasis. Consultant. 2018;58(7):192-193.
A 68-year-old woman presented with epigastric pain and weight loss. She had a history of hydronephrosis and had recently undergone ureteral stent placement with biopsy of an irregular base and posterior portion of the bladder. She had a family history of a brain tumor in her mother. She was an ex-smoker who had quit 25 years prior.
Laboratory test results were significant for a cancer antigen (CA) 19-9 level of 43.2 U/mL (reference value, <37 U/mL) and a CA 125 level of 170 U/mL (reference value, <35 U/mL).
During hospitalization, upper endoscopy showed a friable circumferential 4-cm mass in the cardia extending into the upper gastric body (Figures 1A-1D). Multiple biopsies were performed. Pathology test results showed diffuse-type adenocarcinoma of signet-ring cell carcinoma (SRCC) (Figures 2A-2D). Pathology tests of a urothelial biopsy returned similar results (Figures 3A-3D and 4A-4F). The tumor was negative for the HER2 and gastric PD-L1 cancer biomarker proteins. Immunohistochemical analysis showed no evidence of mismatch repair deficiency.
She was evaluated by an oncologist and was started on oxaliplatin with fluorouracil and folinic acid (FOLFOX) chemotherapy. After completing 1 round as an inpatient, she was discharged home to follow-up as an outpatient.




Figure 1A-1D. Endoscopic images of a 4-cm circumferential mass in the stomach.
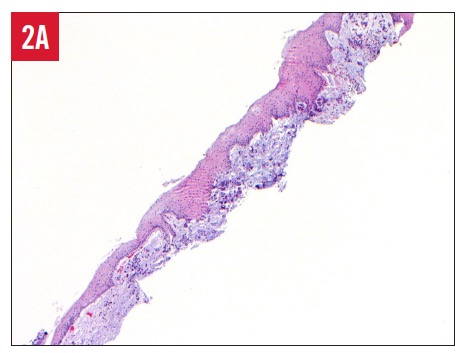



Figure 2. Multiple fields of a gastroesophageal junction biopsy result demonstrating diffuse subepithelial infiltration of signet-ring cells (hematoxylin-eosin; original magnification ×40 [A], ×100 [B], ×200 [C], and ×400 [D]).




Figure 3. Multiple fields of a bladder biopsy result demonstrating diffuse suburothelial infiltration of signet-ring cells (hematoxylin-eosin; original magnification ×40 [A], ×200 [B], and ×400 [C and D]).
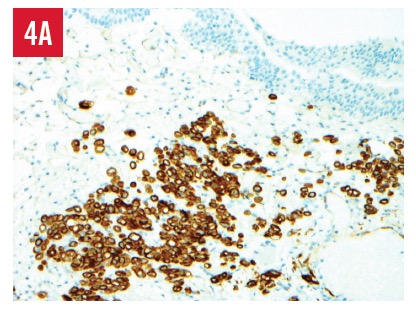





Figure 4. Cytokeratin 7 stain, positive (A); cytokeratin 20 stain, positive (B); villin stain, positive (C); CDX2 stain, negative (D); mucicarmine stain, positive (E); and Ki-67 stain, >90% positive (F). Original magnification ×200.
NEXT: Discussion
Discussion. Gastric cancer is the third leading cause of cancer-related death worldwide, with classification based on histology types including tubules, papillae, mucous lakes, solid lesions, and undifferentiated epithelia.1 The 2 main types of gastric adenocarcinoma are intestinal and diffuse.2 Among the diffuse carcinoma types is SRCC.
SRCC arises in the mucosa, infiltrating the lamina propria mucosae, whereby the intracytoplasmic mucin compresses the nucleus of the cell, giving the characteristic signet-ring appearance.3,4 Early gastric SRCC tends to be depressed, with endoscopic detection often occurring with the use of contrast with indigo carmine solution.5 SRCC is a predictor of poorer prognosis among gastric cancers,6 and it is characterized as a high-grade tumor by the World Health Organization.7 In one study of 3104 patients in South Korea undergoing gastrectomy for histologically proven gastric cancer, 566 (17.9%) had SRCC.8
Gastric SRCC presents at a younger age than gastric adenocarcinoma and is more common in black, Asian/Pacific Islander, American Indian/Alaska Native, and Hispanic populations.9 Hereditary predisposing factors were found with CDH1 (which is located on 16q22.1 and encodes E-cadherin, responsible for cell polarity and cell-cell interaction), prompting prophylactic gastrectomies.10
Primary SRCC has been reported in the bladder.11 Our case illustrates a case of SRCC originating in the stomach and metastasizing to the bladder. The pathogenesis may be similar to cases of Krukenberg tumor—a metastatic ovarian signet-ring cell tumor with its primary site usually in the gastrointestinal tract—in which transcoelomic seeding is hypothesized as the mechanism of spread12; however, more research is required to elucidate the pathogenesis.
REFERENCES:
- Rugge M, Fassan M, Graham DY. Epidemiology of gastric cancer. In: Strong VE, ed. Gastric Cancer: Principles and Practice. New York, NY: Springer; 2015:22-34.
- Laurén P. The two histological main types of gastric carcinoma: diffuse and so-called intestinal-type carcinoma: an attempt at a histo-clinical classification. Acta Pathol Microbiol Scand. 1965;64(1):31-49.
- Maehara Y, Sakaguchi Y, Moriguchi S, et al. Signet ring cell carcinoma of the stomach. Cancer. 1992;69(7):1645-1650.
- Nakamura K, Sugano H, Takagi K. Carcinoma of the stomach in incipient phase: its histogenesis and histological appearances. Gan. 1968;59(3):251-258.
- Otsuji E, Yamaguchi T, Sawai K, Takahashi T. Characterization of signet ring cell carcinoma of the stomach. J Surg Oncol. 1998;67(4):216-220.
- Piessen G, Messager M, Leteurtre E, Jean-Pierre T, Mariette C. Signet ring cell histology is an independent predictor of poor prognosis in gastric adenocarcinoma regardless of tumoral clinical presentation. Ann Surg. 2009;250(6):878-887.
- Watanabe H, Jass JR, Sobin LH. Histological classification of oesophageal tumours. In: Watanabe H, Jass JR, Sobin LH. Histological Typing of Oesophageal and Gastric Tumours. 2nd ed. Berlin, Germany: Springer-Verlag; 1990:5-6.
- Hyung WJ, Noh SH, Lee JH, et al. Early gastric carcinoma with signet ring cell histology. Cancer. 2002;94(1):78-83.
- Taghavi S, Jayarajan SN, Davey A, Willis AI. Prognostic significance of signet ring gastric cancer. J Clin Oncol. 2012;30(28):3493-3498.
- Guggenheim DE, Shah MA. Gastric cancer epidemiology and risk factors. J Surg Oncol. 2013;107(3):230-236.
- Yamada Y, Yamada H, Miyagawa Y, et al. A case of signet ring cell carcinoma of the urinary bladder [in Japanese]. Hinyokika Kiyo. 1989;35(7):1207-1211.
- Shah B, Tang W-H, Karn S. Transcoelomic spread and ovarian seeding during ovulation: a possible pathogenesis of Krukenberg tumor. J Cancer Res Ther. 2017;13(1):152-153.