Peer Reviewed
What Is the Cause of This Left Lower Quadrant Pain in an 11-Year-Old Girl?
Answer: D. Fallopian tube torsion
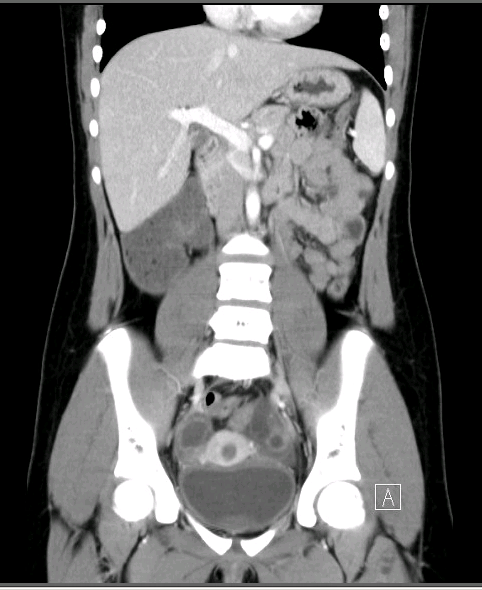
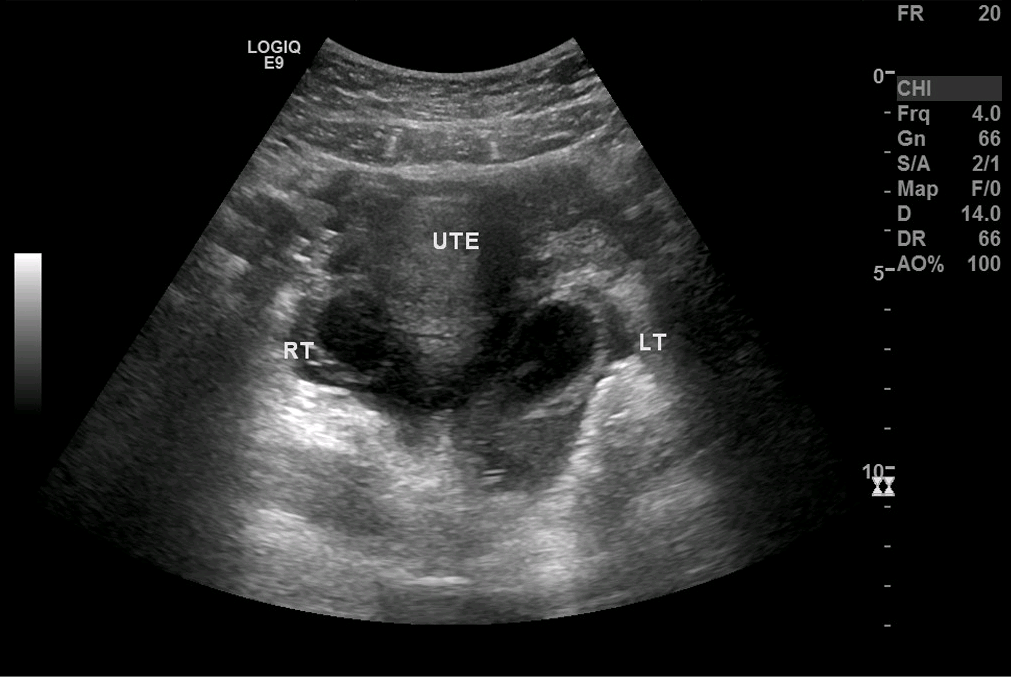
A tortuous tubular structure in the left adnexa raised suspicion for an isolated fallopian tube torsion (Figure 1). Results of an abdominal pelvic computed tomography scan confirmed a diagnosis of left fallopian tube torsion (Figure 2). The abnormal tubular structure was again visualized in the left adnexal region. The tubular diameter measured almost 2 cm. There was free fluid in the pelvis that was seen physiologically.

Discussion. Unilateral fallopian tube torsion is a very uncommon cause of lower abdominal pain.1 The anatomy of this torsion is due to the fixation of the fallopian tube in the left side of pelvis by the sigmoid colon and mesentery.2
Isolated fallopian tube torsion is the rotation of the tube around its longitudinal axis. Bland Sutton first described this condition in 1890.3 The prevalence of this condition is 1 in 1.5 million adult women and is even rarer in children, with only a few cases reported in the literature.4,5
Classically, fallopian tube torsion presents similarly to other conditions, such as ovarian torsion or appendicitis. Pain in the pelvis associated with anorexia, nausea, and vomiting may be the primary symptoms. Ultrasonography and computed tomography scans are the primary modalities for diagnosis.
In pelvic pain cases, the differential diagnoses are various because of the several anatomical structures involved. Specifically, the differential diagnosis can include Mittelschmerz syndrome, ruptured tubal cyst, ruptured ectopic pregnancy, and inflammatory conditions of the pelvic structure.
Because results of the patient’s urine pregnancy test were negative, and she denied sexual activity, both ectopic pregnancy and pelvic inflammatory disease were ruled out.
The definitive treatment for fallopian tube torsion is laparoscopy with detorsion or salpingectomy.
Conclusion. This case demonstrates the importance of an accurate and timely diagnosis of fallopian tube torsion. Although fallopian tube torsion is rare, this case reminds practitioners that ovarian torsion, which is far more common than fallopian tube torsion, is not the only form of torsion to be considered in girls with lower abdominal pain. The occurrence of sudden onset nausea and vomiting without infectious symptoms should prompt the physician to consider torsion of other luminal structures in the female pelvis to include the fallopian tubes. If misdiagnosed or improperly managed, patients can experience lasting effects. However, with the proper diagnosis and treatment, patients can recover and have good clinical outcomes.
Furthermore, lower abdominal pain specially over the left iliac fossa should prompt for further evaluation of fallopian tube torsion, hydrosalpinx, or any pelvic organ inflammation. Findings of hydrosalpinx with pain, especially in a patient who is not sexually active, should prompt further evaluation and possible admission to the hospital for observation with serial abdominal examinations. Treatment is guided by the suspected diagnosis.
Patient outcome. Our patient was taken to the operating room for diagnostic laparoscopy. Findings during surgery were an enlarged necrotic left fallopian tube with evidence of torsion and a normal-appearing left ovary. After surgery, the patient was discharged home in stable condition.
References
1. Comerci G, Colombo FM, Stefanetti M, Grazia G. Isolated fallopian tube torsion: a rare but important event for women of reproductive age. Fertil Steril. 2008;90(4):1198.e23-1198.e25. https://doi.org/10.1016/j.fertnstert.2007.08.057
2. Gross M, Blumstein SL, Chow LC. Isolated fallopian tube torsion: a rare twist on a common theme. AJR Am J Roentgenol. 2005;185(6):1590-1592. https://doi.org/10.2214/ajr.04.1646
3. Bland Sutton J. Remarks on salpingitis and some of its effects. Lancet. 1890;136(3510):1206-1209. https://doi.org/10.1016/S0140-6736(01)86101-8
4. Hansen OH. Isolated torsion of the Fallopian tube. Acta Obstet Gynecol Scand. 1970;49(1):3-6. https://doi.org/10.3109/00016347009157506
5. Terada Y, Murakami T, Nakamura S, et al. Isolated torsion of the distal part of the fallopian tube in a premenarcheal 12 year old girl: a case report. Tohoku J Exp Med. 2004;202(3):239-243. https://doi.org/10.1620/tjem.202.23