
Peer Reviewed
Bladder Injury Mimicking Acute Kidney Injury
Authors:
Katlyn Baxter, DO; Ryan Lauf, DO; and Kim Jordan, MD
OhioHealth Riverside Methodist Hospital, Columbus, Ohio
Citation:
Baxter K, Lauf R, Jordan K. Bladder injury mimicking acute kidney injury. Consultant. 2018;58(8):215-117.
A 27-year-old woman underwent uncomplicated laparoscopic right oophorectomy for a dermoid ovarian cyst. Her postprocedural recovery had been uneventful, and she had been discharged home the same day. Over the following week, she had noticed increasing abdominal distention, diffuse abdominal pain, severe nausea, and poor oral intake. She also reported having little to no urine output for approximately 3 days. Her only medication had been oxycodone-acetaminophen, which had been prescribed for postprocedural pain. The patient’s symptoms prompted presentation to an emergency department (ED) 6 days after the procedure.
Physical examination. At presentation in the ED, the patient was hemodynamically stable. Physical examination findings were positive for a diffusely tender, distended abdomen. There was no peripheral edema, and cardiopulmonary examination findings were unremarkable.
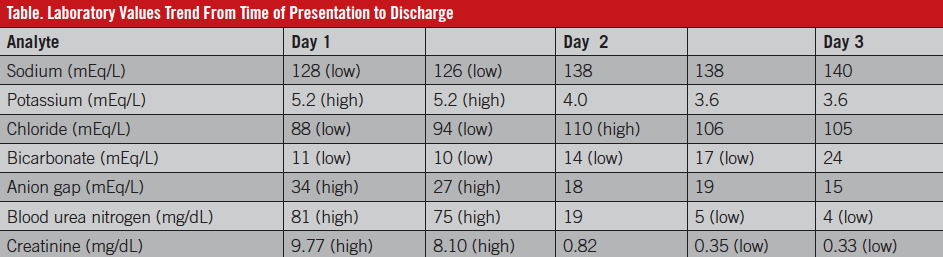
Diagnostic tests. Initial laboratory studies found hyponatremia of 128 mEq/L, hyperkalemia of 5.2 mEq/L, a low bicarbonate level of 11 mEq/L, an elevated anion gap of 34 mEq/L, and an elevated serum creatinine level of 9.77 mg/dL with an elevated blood urea nitrogen (BUN) level of 81 mg/dL. Urinalysis results were significant for 30 mg/dL of protein, 80 or more mg/dL of ketones, a small amount of blood, leukocyte esterase, and 1 granular cast but no nitrites. The platelet count and the international normalized ratio were normal.
The differential diagnosis included postoperative complications including obstructive uropathy, dehydration with resultant prerenal acute kidney injury (AKI), medication-induced AKI, pyelonephritis, interstitial nephritis, nephrotic syndrome, tubular dysfunction, and pancreatitis. Other diagnostic considerations in patients presenting with ascites and renal failure, although not likely in this patient, are cirrhosis with hepatorenal syndrome, heart failure or constrictive pericarditis with cardiorenal syndrome, malignancy, infections (eg, tuberculosis), abdominal compartment syndrome, and systemic capillary leak syndrome.
A urinary catheter was placed, resulting in the immediate return of 200 mL of clear fluid; however, over the next 2 hours, urine output was 1300 mL. Computed tomography (CT) of the abdomen and pelvis revealed protrusion of the urinary catheter through the dome of the bladder into the intraperitoneal space, large ascites, and free intraperitoneal air (Figures 1 and 2). The liver and kidneys appeared normal; there was no hydronephrosis (Figure 3).

Figure 1: CT of the abdomen and pelvis demonstrating perforation of a urinary catheter through the dome of the bladder.

Figure 2: CT of the abdomen and pelvis, lateral view, showing perforation of a urinary catheter through the dome of the bladder and free intraperitoneal air.
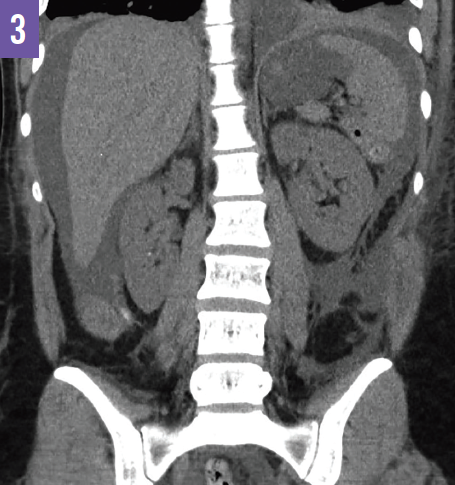
Figure 3: CT of the abdomen and pelvis demonstrating ascites and normal kidneys without evidence of hydronephrosis.
Treatment. The patient was transferred to our facility for emergent surgery, which revealed 2 injuries to the bladder, 1 anteriorly and 1 posteriorly, immediately below the suprapubic port site incision, suggesting a trocar injury to the bladder. A copious amount of clear fluid was drained from the peritoneum consistent with urinary ascites.
Outcome of the case. Within 24 hours of surgical repair, the patient’s abdominal pain and distention had significantly improved, and she had normal urine output and a normal serum creatinine level of 0.82 mg/dL with a BUN level of 19 mg/dL (Table). Electrolyte levels and the anion gap also normalized within 48 hours. She was discharged home on postoperative day 2. A follow-up cystogram at 2 weeks demonstrated normal bladder without contrast extravasation or mass.
Discussion. AKI is an abrupt and potentially reversible decline in the glomerular filtration rate, with resultant elevated levels of BUN and serum creatinine as well as other metabolic waste products. The Acute Kidney Injury Network criteria for AKI include the following: 1) an absolute increase in serum creatinine of 0.3 mg/dL or greater from baseline; 2) an increase in the serum creatinine concentration of 50% or greater; or 3) oliguria of less than 0.5 mL/kg/h for 6 hours.1 An estimated 7% of hospitalized patients experience AKI, and the degree of elevation of serum creatinine is correlated with higher mortality rates.2 The multiple etiologies for AKI are typically organized into categories of prerenal, intrinsic renal and postrenal causes.
This case reminds clinicians to consider bladder injury in patients presenting with postoperative ascites and clinical and laboratory parameters suggestive of AKI. Although our patient’s symptoms were consistent with uremia, her markedly elevated creatinine and BUN levels were related to peritoneal absorption of urea and creatinine from urinary ascites due to bladder injury, previously referred to as “reverse auto-dialysis” or “pseudo-AKI.”3-7 The metabolic derangements associated with urinary ascites underscore the importance of early identification and correction of the bladder injury. Our patient required treatment with sodium bicarbonate, but dialysis was not necessary. Indeed, her kidneys actually functioned normally, evidenced by rapid normalization of serum creatinine and BUN following surgical repair. Lack of hydronephrosis on imaging ruled out an obstructive etiology.
The incidence of urinary tract injury associated with pelvic surgery in women ranges between 0.3% and 1%. Bladder injury is more common than ureteral injury.8 Abdominal or pelvic surgery, blunt abdominal trauma (usually accompanied by pelvic fracture),9 and pelvic irradiation10 are the more commonly cited causes of bladder rupture, but spontaneous rupture has also been reported following vaginal deliveries6,11 and in cases of chronic inflammation or neurogenic bladder.12
With regard to iatrogenic surgical injury, the average reported delay from incident to presentation is 5.4 days if the injury is not identified intraoperatively.13 Cases have been reported in which the diagnosis was dramatically delayed. One case report described transurethral resection of a bladder tumor complicated by small-volume, self-resolving leaks that recurred over several months, causing urinary ascites and metabolic derangements.7 Another report describes a case of spontaneous bladder rupture during delivery, but the jejunum sealed off the injury for nearly a month before the patient presented with abdominal pain, distention, and oliguria.11 Thus, obtaining a thorough history is emphasized. Patients should undergo immediate repair to decrease the risk of metabolic abnormality from reverse autodialysis, the risk of peritonitis and sepsis,14 or the unnecessary initiation of dialysis or medications.
CT cystography is the most sensitive and accurate diagnostic test for bladder injury.15 Evaluation of BUN, creatinine, and potassium in the ascitic fluid and calculation of an ascites-to-serum creatinine ratio can be used to diagnose ascites. A ratio greater than 1 and ascitic urea, creatinine, and potassium levels that resemble serum levels are suggestive of urinary ascites.7
References:
- Mehta RL, Kellum JA, Shah SV, et al; Acute Kidney Injury Network. Acute Kidney Injury Network: report of an initiative to improve outcomes in acute kidney injury. Crit Care. 2007;11(2):R31.
- Nash K, Hafeez A, Hou S. Hospital-acquired renal insufficiency. Am J Kidney Dis. 2002;39(5):930-936.
- Abirami K, Sivaramakrishna G, Lakshmi AY, Sivakumar V. Urinary ascites. Indian J Nephrol. 2012;22(2):143-144.
- Aber A, Hyder SA, Arumuham V. An unusual case of spontaneous bladder perforation with associated autodialysis of the ensuing urinary ascites. Case Rep Med. 2011;2011:145084.
- Shah R, Ramakrishnan M, Ahmed B, Abuamr K, Yousef O. Perforated bladder as a cause of abdominal ascites in a patient presenting with acute onset abdominal pain. Cureus. 2017;9(5):e1241.
- Charalampidis S, Petrides C, Charalampous C, Stavrou S. Hyponatremic renal pseudofailure and massive ascites following normal vaginal delivery: a diagnostic and therapeutic challenge. Ren Fail. 2012;34(2):237-240.
- Matsumura M, Ando N, Kumabe A, Dhaliwal G. Pseudo-renal failure: bladder rupture with urinary ascites. BMJ Case Rep. 2015. doi:10.1136/bcr-2015-212671
- Teeluckdharry B, Gilmour D, Flowerdew G. Urinary tract injury at benign gynecologic surgery and the role of cystoscopy: a systematic review and meta-analysis. Obstet Gynecol. 2015;126(6):1161-1169.
- Kong JPL, Bultitude MF, Royce P, Gruen RL, Cato A, Corcoran NM. Lower urinary tract injuries following blunt trauma: a review of contemporary management. Rev Urol. 2011;13(3):119-130.
- Goto S, Yamadori M, Igaki N, Kim JI, Fukagawa M. Pseudo-azotaemia due to intraperitoneal urine leakage: a report of two cases. NDT Plus. 2010;3(5):474-476.
- Farahzadi A, Mohammadipour S. A late presentation of spontaneous bladder rupture during labor. Urol Case Rep. 2016;8:24-25.
- Craggs B, Michielsen D. Conservative treatment of an intraperitoneal bladder perforation. Cent European J Urol. 2011;64(1):47-49.
- Mokoena T, Naidu AG. Diagnostic difficulties in patients with a ruptured bladder. Br J Surg. 1995;82(1):69-70.
- Esparaz AM, Pearl JA, Herts BR, LeBlanc J, Kapoor B. Iatrogenic urinary tract injuries: etiology, diagnosis, and management. Semin Intervent Radiol. 2015;32(2):195-208.
- Deck AJ, Shaves S, Talner L, Porter JR. Computerized tomography cystography for the diagnosis of traumatic bladder rupture. J Urol. 2000;164(1):43-46.