
Peer Reviewed
Invasive Haemophilus influenzae Type F Infection Complicated by Subarachnoid Phlegmon and Cortical Venous Thrombosis
AUTHORS:
Camila De Avila, MD • Kyle Pipkin, DO • William Novotny, MD
AFFILIATION:
East Carolina University/Vidant Medical Center, Greenville, North Carolina
CITATION:
De Avila C, Pipkin K, Novotny W. Invasive Haemophilus influenzae type F infection complicated by subarachnoid phlegmon and cortical venous thrombosis. Consultant. 2021;61(12):e27-e30. doi:10.25270/con.2021.03.00009
Received October 8, 2020. Accepted January 11, 2021. Published online March 15, 2021.
DISCLOSURES:
The authors report no relevant financial relationships.
CORRESPONDENCE:
Camila De Avila, MD, East Carolina University/Vidant Medical Center, 600 Moye Boulevard, Vidant Medical Annex 215, Greenville, NC 27834 (camiladeavilamd@gmail.com)
A 7-month-old boy with macrocephaly presented to our emergency department with a fever and left-sided otitis media. He had not been immunized against influenza but was otherwise healthy. He also had no history of infections and was growing normally.
Diagnostic testing. Diagnostic testing revealed the source of the boy’s fever was influenza type B. Amoxicillin and oseltamivir were prescribed at that time, and the boy was discharged home.
Three days later, the patient presented again for irritability, reduced activity, and respiratory distress associated with right upper lobe superimposed pneumonia. Amoxicillin-clavulonic acid was prescribed at discharge one day later, and oseltamivir was continued for the full 5-day course. During this brief admission, a blood culture was collected, which grew Haemophilus influenza type f (Hif) β-lactamase negative.
The next day the patient presented with incessant crying, persistent fever, and jerking movements of the extremities on the right side. The patient was then was readmitted to the hospital.
Cerebrospinal fluid (CSF) analysis revealed elevated levels of nucleated cells at 35/mcL with 45% neutrophils, 47% lymphocytes, and 8% monocytes; low level of red blood cells at 4/mcL; decreased CSF glucose level at 47 mg/dL; and normal level of CSF proteins at 41 mg/dL. Organisms were not detected on a Gram stain of the CSF, and results of a meningitis encephalitis panel were negative, including H influenzae polymerase chain reaction assay. A computed tomography (CT) scan of the head showed mild prominence of extra-axial spaces, consistent with benign enlargement of the subarachnoid spaces of infancy. Bacterial growth was not seen on the CSF analysis or on a repeat blood culture. The patient was started on intravenous (IV) ceftriaxone, 100 mg/kg/d, and phenobarbital for seizure management.
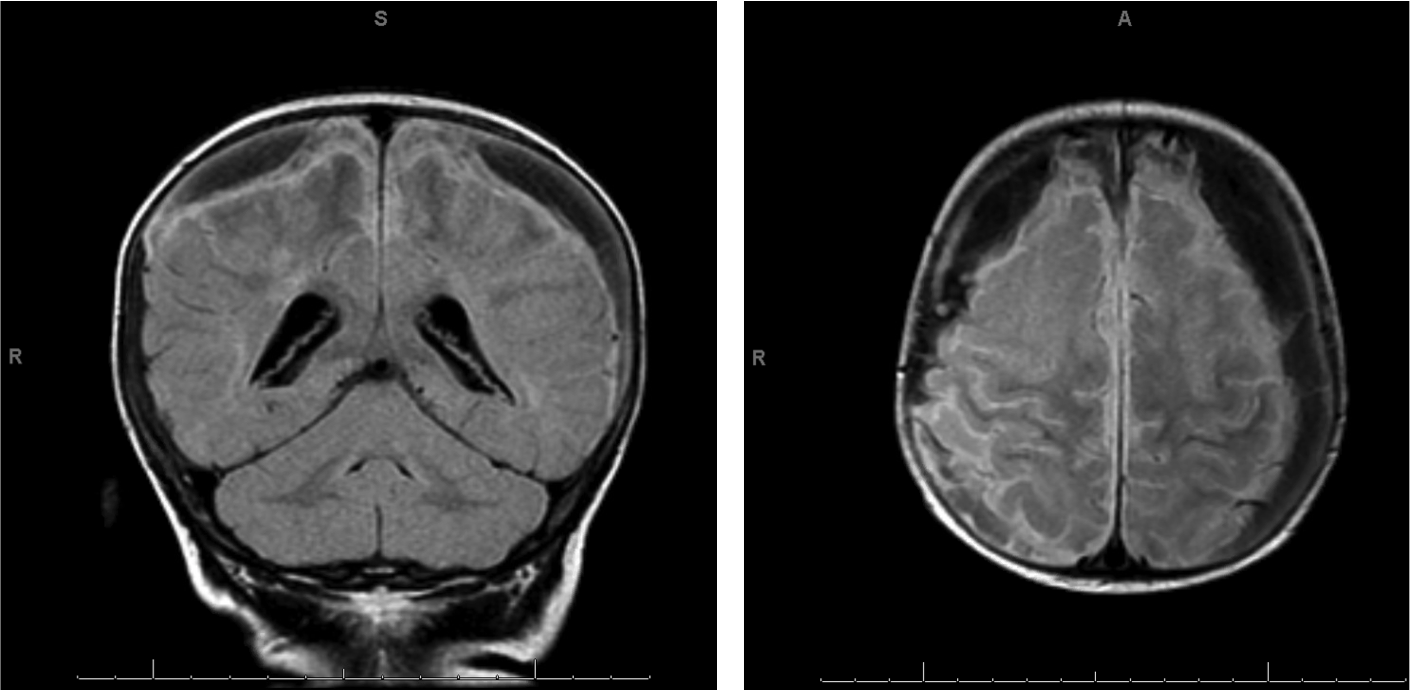
Three days later, despite a therapeutic phenobarbital level, the patient had a prolonged partial clonic seizure of the left lower extremity that resolved after treatment with lorazepam and extra doses of phenobarbital. A magnetic resonance imaging (MRI) scan of the brain on the day of the seizure showed severe, diffuse leptomeningeal thickening, enhancement of bilateral cerebral hemispheres, and bilateral “subdural fluid collections” (Figure 1). These presumed subdural empyemas were associated with mass effect on the underlying brain but were not associated with transtentorial herniation or hydrocephalus. Immediately, bilateral burr hole craniotomies were performed, and subdural drains were placed.
During the surgical procedure to place the drains, solid phlegmon was visualized in the subarachnoid space that could not be removed by suction. On hospital day 4, left upper and lower extremity paresis were noted. An electroencephalogram (EEG) revealed no seizure activity. On hospital day 6, after 3 days of extra-axial drainage, a repeat head MRI scan showed new left frontal cortical venous thrombosis with normal signal in the subadjacent brain parenchyma. Subsequently, enoxaparin was started as anticoagulation therapy. At this time, the patient was also noted to have thrombocytosis with a platelet level of 1214 k/uL and was initiated on aspirin as well.
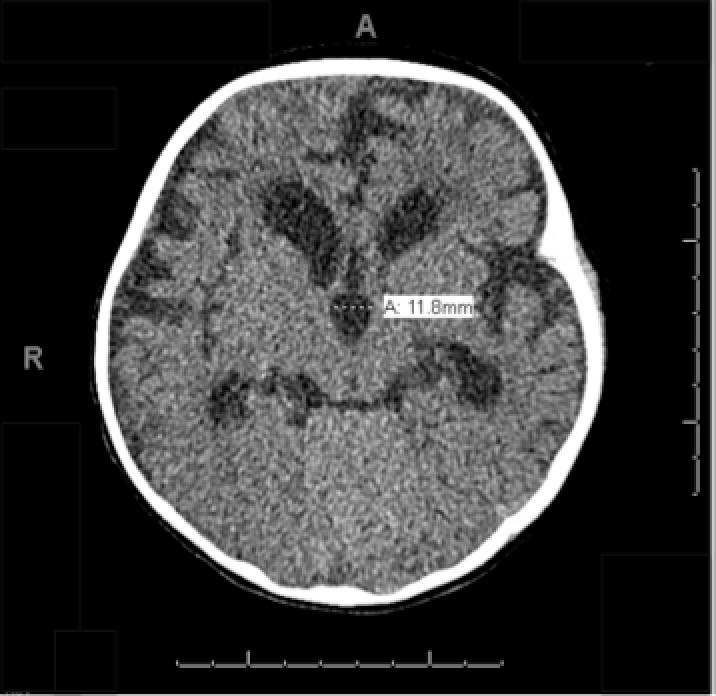
Extra-axial drainage was steady for a 10-day period. A repeat head CT scan on hospital day 10 revealed dilatation of the cerebral ventricles (Figure 2). Therefore, the bilateral subdural drains were removed, and an external ventricular drain was placed and remained in place for 12 days.
By hospital day 10, the patient’s left upper extremity had minimal motor function, but the left lower extremity had no motor function. During the hospital course, further workup revealed a normal protein C level of 75% (reference range, 70%-180%) and normal protein S level of 72% (reference range, 70%-150%). IV ceftriaxone was continued for a 1-month course. Three weeks after admission, the patient’s immunoglobulin (Ig) levels were measured. IgA, IgG, and IgM levels were all within normal limits.
The patient was discharged to our hospital’s rehabilitation service approximately 1 month after admission with an extended course of aspirin and therapeutic enoxaparin. His motor function was still impaired in his extremities on the left side.
After a subsequent 2-week rehabilitation stay, the patient continued to have residual motor deficits that required physical and occupational therapy. Because hearing loss is common among patients with Hif infections, a tympanometry was performed, results of which demonstrated normal hearing function bilaterally.
Discussion. H influenzae is strictly a human pathogen, gram-negative coccobacillus, which usually infects the upper respiratory tract and can cause serious invasive infections, especially in children younger than 5 years.1-8 There are 6 encapsulated serotypes characterized by distinctive capsular polysaccharides (a-f), as well as 3 nonencapsulated or nontypeable strains.2,3,7 In 1994, invasive Hif was reported to occur at frequency of 1.9 cases per 1 million children with pneumonia and meningitis being the most common presentations.9
The percentage of Hif infections has declined with universal introduction of the conjugate vaccine.10 With this decline, the incidence of invasive infections caused by nontypeable or other strains of H influenzae,5,7,11 particularly serotype f, has grown in the United States as well as other countries.12-14 In the pediatric population, pneumonia and meningitis are the most common forms of severe Hif infection.1,8 Interestingly, the majority of invasive non-typeable Hif cases occur in immunocompetent patients who have no predisposing risk factors.7 Nontypeable H influenzae vaccines are currently under investigation.6
Since the Hif conjugate vaccine was introduced in 1990, most invasive illnesses in US children, specifically bacteremia and meningitis, have been due to either nontypeable strains or non-Hif capsular serotypes.1,7,11,14 Viral respiratory coinfections, like with influenza B virus seen in our patient, can have a synergistic effect to increase the virulence of these bacteria, facilitating both the focal spread and systemic invasion, and increasing morbidity and mortality.4
Conclusions. Here we have presented a case of a 7-month-old boy with no apparent underlying disease, who presented to our clinic with influenza B viral infection and Hif bacteremia associated with pneumonia and meningitis. Intracranial complications included bilateral subdural empyemas and cortical venous thrombosis. Initial treatment included oral antiviral and antibacterial therapy, but the presence of fever, irritability, and seizures prompted a second medical evaluation. Clinical presentation and growth of Hif from the blood culture taken during one of the initial medical evaluations prompted a CSF analysis. The results revealed no organisms on Gram stain and no bacterial growth. However, the presence of 35 nucleated cells with 45% neutrophils was concerning for infectious bacterial meningitis caused by Hif. The head CT scan performed before the spinal tap revealed mildly prominent extra-axial spaces over the nondependent fronto-parietal lobes, consistent with benign enlargement of subarachnoid spaces of infancy. It is unknown whether this extra space for CSF accumulation may have predisposed the infant to develop bacterial meningitis and phlegmons.
The initial brain MRI was performed on day 3 of the second hospitalization and was notable for severe diffuse leptomeningeal thickening and enhancement overlying the bilateral cerebral hemispheres. On hospital day 4, left upper and lower extremity paresis was observed. When paresis persisted, a second brain MRI scan was conducted on hospital day 6. No structural right-sided lesions were appreciated on the MRI scan that could readily explain the left-sided paresis. Instead, a newly visualized left-sided frontal cortical venous thrombosis was present. In retrospect and conversely, clinically evident right upper and lower extremity seizures were present at the time of the second admission. It is possible that left-sided brain injury or inflammation related to Hif bacterial meningitis caused these early seizures. Perhaps, a nidus for an evolving left-sided thrombus, which was not visible until hospital day 6, was already present on hospital day 3 and triggered focal right-sided seizure activity. The prolonged paresis and unremarkable results of an electroencephalography suggests that subclincal seizure activity and postictal paresis15 were unlikely explanations for paresis.
Unremarkable Ig levels and the absence of history of prior infections in an infant who was growing normally implied the presence of intact immunocompetency. Rather, the occurrence of meningitis, bacteremia, pneumonia, subarachnoid phlegmons, focal seizures, prolonged focal neurological deficits, and cortical venous thrombosis underscored the virulence of Hif.
Typeable and nontypeable H influenzae commonly colonize respiratory mucosa in children, which constitute the first step of its pathogenesis. In addition, the presence of other infections, such as acute otitis media or rhinosinusitis, can facilitate direct extension along the respiratory mucosa to a new site.16 Furthermore, in our patient, normal immune function may have been compromised because of a primary viral infection with influenza B virus that may have been predisposed to pneumonia and bacteremia. The bacteremia in turn may have seeded the pre-existing prominent subarachnoid spaces after being introduced into the CSF by passing through the choroid plexus.17 An oral antibiotic was predictably insufficient to fully treat the Hif meningitis,11,18 and complications ensued.
Patient outcome. Our patient was discharged home after a 2-week course of inpatient pediatric rehabilitation. He continued receiving weekly outpatient physical and occupational therapy with improvements in his motor strengths. For his seizures, he was continued on phenobarbital. The results of a repeat EEG a month after discharge were normal, with no seizure activity detected. Enoxaparin and aspirin were continued to complete a 3-month regimen of anticoagulation.
- Abou-Hanna J, Panning K, Mehta H. Haemophilus influenza type f meningitis complicated by bilateral subdural empyema, central venous thrombosis, and bilateral sensorineural hearing loss in an immunocompetent 12-month-old. Cureus. 2019;11(6):e4850. https://doi.org/10.7759/cureus.4850
- Oikonomou K, Alhaddad B, Kelly K, Rajmane R, Apergis G. Haemophilus influenzae serotype f endocarditis and septic arthritis. IDCases. 2017;9:79-81. https://doi.org/10.1016/j.idcr.2017.06.008
- Ladhani SN, Collins S, Vikers A, et al. Invasive Haemophilus influenzae serotype e and f disease, England and Wales. Emerg Infect Dis. 2012;18(5):725-732. https://doi.org/10.3201/eid1805.111738
- Lee LN, Dias P, Han D, et al. A mouse model of lethal synergism between influenza virus and Haemophilus influenzae. Am J Pathol. 2010;176(2):800-811. https://doi.org/10.2353/ajpath.2010.090596
- Thorgrimson J, Ulanova M. Haemophilus influenzae type a as a cause of paediatric septic arthritis. JMM Case Rep. 2016;3(5):e005064. https://doi.org/10.1099/jmmcr.0.005064
- Murphy TF. Vaccines for nontypeable Haemophilus influenzae: the future is now. Clin Vaccine Immunol. 2015;22(5):459-466. https://doi.org/10.1128/cvi.00089-15
- Antony S, Kaushik A, Mauriello C, Chatterjee A. Non–type b Haemophilus influenzae invasive infections in North Dakota and South Dakota, 2013–2015. J Pediatric Infect Dis Soc. 2017;6(3):281-284. https://doi.org/10.1093/jpids/piw053
- O'Neill JM, St Geme 3rd JW, Cutter D, et al. Invasive disease due to nontypeable Haemophilus influenzae among children in Arkansas. J Clin Microbiol. 2003;41(7):3064-3069. https://doi.org/10.1128/jcm.41.7.3064-3069.2003
- Urwin G, Krohn JA, Deaver-Robinson K, Wegner JD, Farley MM. Invasive disease due to Haemophilus influenaze serotype f: clinical and epidemiologic characteristics in the H. influenzae serotype b vaccine era. The Haemophilus influenzae Study Group. Clin Infect Dis. 1996;22(6):1069-1076. https://doi.org/10.1093/clinids/22.6.1069
- Adams WG, Deaver KA, Cochi SL, et al. Decline of childhood Haemophilus influenzae type b (Hif) disease in the Hif vaccine era. JAMA. 1993;269(2):221-226. doi:10.1001/jama.1993.03500020055031
- Vallejo JG, McNeil JC, Hultén KG, Sommer LM, Dunn JJ, Kaplan SL. Invasive Haemophilus influenzae disease at Texas Children’s Hospital, 2011 to 2018. Pediatr Inf Dis J. 2019;38(9):900-905. https://doi.org/10.1097/inf.0000000000002383
- Suga S, Ishiwada N, Sasaki Y, et al. A nationwide population-based surveillance of invasive Haemophilus influenzae diseases in children after the introduction of the Haemophilus influenzae type b vaccine in Japan. Vaccine. 2018;36(38):5678-5684. https://doi.org/10.1016/j.vaccine.2018.08.029
- Whittaker R, Economopoulou A, Dias JG, Bancroft E, Ramliden M, Celentano LP; European Centre for Disease Prevention and Control Country Experts for Invasive Haemophilus influenzae Disease. Epidemiology of invasive Haemophilus influenzae disease, Europe, 2007-2014. Emerg Infect Dis. 2017;23(3):396-404. https://doi.org/10.3201/eid2303.161552
- Soeters HM, Blain A, Pondo T, et al. Current epidemiology and trends in invasive Haemophilus influenzae disease-United States, 2009-2015. Clin Infect Dis. 2018;67(6):881-889. https://doi.org/10.1093/cid/ciy187
- Rolak LA, Rutecki P, Ashizawa T, Hrati Y. Clinical features of Todd’s post-epileptic paralysis. J Neurol Neurosurg Psychiatry. 1992;55(1):63-64. https://doi.org/10.1136/jnnp.55.1.63
- Thors V, Christensen H, Morales-Aza B, et al. High-density bacterial nasal carriage in children is transient and associated with respiratory viral infections-implications for transmission dynamics. Pediatr Infect Dis J. 2019;38(5):533-538. https://doi.org/10.1097/inf.0000000000002256
- Soeters HM, Blain A, Pondo T, et al. Current epidemiology and trends in invasive Haemophilus influenzae disease-United States, 2009-2015. Clin Infect Dis. 2018;67(6):881-889. https://doi.org/10.1093/cid/ciy187
- Haemophilus influenzae infections. In: Kimberlin DW, Long SS, Brady MT, Jackson MA, eds. Red Book: 2018-2021 Report of the Committee on Infectious Diseases. 31st ed. American Academy of Pediatrics; 2018:367-375.