
Peer Reviewed
Complications from an Atypical Presentation of a Cholecystoduodenal Fistula
AUTHORS:
Muhammad Danial, DO1 • Mansoor Choudhry, DO1 • Matthew K. Creech, DO1 • Ariel Rodriguez, MD2 • Syed A. A. Rizvi, PhD, MS, MBA3
AFFILIATIONS:
1Dr. Kiran C. Patel College of Osteopathic Medicine, Nova Southeastern University, Fort Lauderdale, Florida
2Bethesda Hospital, Boynton Beach, Florida
3Hampton University School of Pharmacy, Hampton, Virginia
CITATION:
Danial M, Choudhry M, Creech MK, Rodriguez A, Rizvi SAA. Complications from an atypical presentation of a cholecystoduodenal fistula. Consultant. 2020;60(6):e5. doi:10.25270/con.2020.05.00006
Received December 11, 2019. Accepted March 24, 2020.
DISCLOSURES:
The authors report no relevant financial relationships.
CORRESPONDENCE:
Syed A. A. Rizvi, PhD, MS, MBA, Department of Pharmaceutical Sciences, Hampton University School of Pharmacy, 100 E Queen St, Hampton, VA 23669 (syed.rizvi@hamptonu.edu)
A 78-year-old woman presented to the hospital with 1-day history of biliary colic, emesis, and diarrhea. Her medical history was significant for type 2 diabetes with neuropathy, dyslipidemia, and hypertension. There were no signs of bowel obstruction on physical examination. The patient reported having shaking chills but denied having abdominal pain, chest pain, hematemesis, hematochezia, dyspnea, or urinary tract symptoms. She also had mild fever and a positive Murphy sign.
The patient was found to have elevated liver function test (LFT) results, including a total bilirubin level of 3.6 mg/dL (reference range, 0.0-1.4 mg/dL), a direct bilirubin level of 2.1 mg/dL (reference range, 0.0-0.3 mg/dL), an alkaline phosphate level of 145 U/L (reference range, 38-126 U/L), an alanine aminotransferase level of 449 U/L (reference range, 17-63 U/L) and an aspartate aminotransferase level of 505 U/L (reference range, 0-37 U/L).
Abdominal ultrasonography (Figures 1 and 2) showed the gallbladder to be abnormal and completely filled with stones. The gallbladder wall was thickened, measuring up to 7 mm—a finding consistent with acute calculous cholecystitis. No definite fluid was seen in the gallbladder fossa, and no dilated common bile duct was noted.
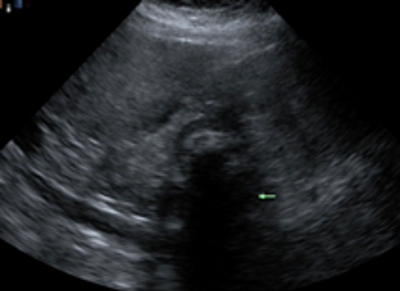
Figure 1. Abdominal ultrasonography showing acoustic shadowing due to the presence of gallstones.
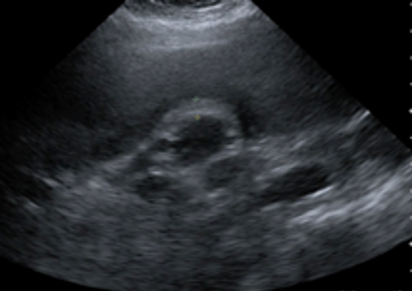
Figure 2. Abdominal ultrasonography showing gallbladder wall thickening.
Given the patient’s elevated LFT results, including an elevated bilirubin suggesting obstruction and concerning for choledocholithiasis, magnetic resonance cholangiopancreatography (MRCP) was performed and confirmed the ultrasonography results (Figure 3). One large gallstone and other smaller stones were present in the gallbladder. There was some minimal fluid in or inflammation in the gallbladder fossa, nonspecific but suggesting cholecystitis. Endoscopic retrograde cholangiopancreatography (ERCP) confirmed the presence of a gallstone and inflammatory findings consistent with acute calculous cholecystitis (Figure 4). No imaging modality gave a clear indication of the presence of a cholecystoenteric fistula (CEF).
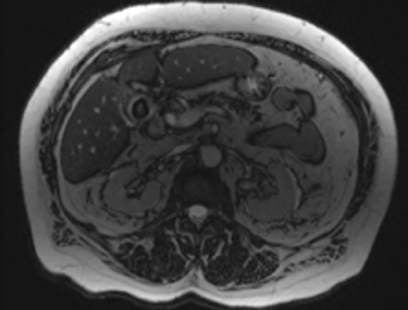
Figure 3. MRCP showing a large gallstone with gallbladder wall inflammation and thickening consistent with the diagnosis of acute cholecystitis. CDF was not identified.

Figure 4. ERCP showing minimal filling defects in the distal common bile duct. No clear evidence of a CDF was seen, since ERCP is limited in terms of providing the anatomical context of the contrast.
A laparoscopic cholecystectomy was performed, but since the duodenum was abnormally adherent to the gallbladder wall, the procedure was converted to open cholecystectomy, during which a cholecystoduodenal fistula (CDF) was observed incidentally and repaired successfully. The significant increase in the duration of surgery, in addition to the patient’s comorbidities, may have contributed to postoperative ventilator-dependent respiratory failure. Furthermore, the patient developed sepsis—a complication for which CEFs are known to carry an increased risk—which led to the development of acute kidney failure due to acute tubular necrosis, necessitating hemodialysis. The patient was transferred to a long-term acute care hospital for further care, and she survived.
DISCUSSION
CEFs are a rare communicating channel between the biliary system and the gastrointestinal tract, are usually complications of gallstone (due to inflammation and increased intracholecystic pressure), and are categorized as internal or external.1 Internal biliary fistulas are rare and occur mostly due to delayed complications of gallstone and without a notable collection of bile. External fistulas are related to trauma to or invasive procedures of the biliary tract and are accompanied with controlled or uncontrolled discharge of bile or bile-containing fluids.2-4 Among the various types of CEFs, CDFs account for the majority (55% to 75%),5 followed by cholecystocolonic fistulas.6
CEFs account for 0.5% to 1.9% of all biliary disease.7 They can occur spontaneously or in association with conditions such as inflammatory bowel diseases and bowel or pancreatic malignancy.8
CEFs are challenging to diagnose preoperatively, since symptoms (eg, abdominal pain, nausea, steatorrhea, diarrhea, etc) often mirror gallbladder disorders.9 Modalities such as abdominal radiography, ultrasonography, barium studies, ERCP, MRCP, computed tomography, percutaneous transhepatic cholangiography, and cholescintigraphy can aid in the preoperative diagnosis of CEF, but they have varying sensitivities and advantages that should be addressed to avoid incidental intraoperative discovery and resultant complications.
However, illustrated by our patient’s case, the radiologic modalities currently used to assess biliary pathology can fail to clearly show a CEF, which puts the surgeon in a peculiar situation, potentially complicating the surgical course of the patient. CEFs are generally managed laparoscopically but carry increased risks of contamination of the peritoneal cavity or prolonged biliary drainage.9 The open approach is necessitated, however, in cases where extensive inflammatory changes have altered the normal anatomy significantly, as in this patient’s case.
This case highlights the importance of having a suspicion for the presence of a CEF, especially when a difficult anatomic dissection is encountered by a surgeon, even without detection of CEF on imaging and absence of gallstone ileus and other typical characteristics of a fistula. The surgeon should take extra steps to ensure the successful discovery and repair of any fistulas. In a patient with multiple comorbidities, it might be helpful for a surgeon to anticipate the presence of such a complication so as to be prepared to complete the surgery as efficiently as possible, saving the patient from the consequences of a prolonged surgery.
REFERENCES:
- Ganapathy TC, Jeyakumar S, Manimaran P, Sekhar S. Laparoscopic management of cholecystoduodenal fistula: a case report. Int Surg J. 2018;5(11):3744-3746. doi:10.18203/2349-2902.isj20184655
- Crespi M, Montecamozzo G, Foschi D. Diagnosis and treatment of biliary fistulas in the laparoscopic era. Gastroenterol Res Pract. 2016;2016:6293538. doi:10.1155/2016/6293538
- Mohammed N, Godfrey EM, Subramanian V. Cholecysto-duodenal fistula as the source of upper gastrointestinal bleeding. Endoscopy. 2013;45(suppl 2):E250-E251. doi:10.1055/s-0033-1344418
- Corvera CU, Jarnagin WR, Blumgart LH. Biliary fistulae. In: Jarnagin WR, Belghiti J, Büchler MW, et al, eds. Blumgart’s Surgery of the Liver, Biliary Tract, and Pancreas. Vol 1. 5th ed. Elsevier; 2012:644-669.
- Ibrahim IM, Wolodiger F, Saber AA, Dennery B. Treatment of cholecystocolonic fistula by laparoscopy. Surg Endosc. 1995;9(6):728-729. doi:10.1007/bf00187951
- Costi R, Randone B, Violi V, et al. Cholecystocolonic fistula: facts and myths. A review of the 231 published cases. J Hepatobiliary Pancreat Surg. 2009;16(1):8-18. doi:10.1007/s00534-008-0014-1
- Pei F, Liu Y, Zhang F, Li N, Huang D, Gu B. Cholecystoduodenal fistula: ultrasonographic diagnosis with oral gastrointestinal ultrasound contrast medium. Abdom Imaging. 2011;36(5):561-564. doi:10.1007/s00261-010-9661-1
- Balent E, Plackett TP, Lin-Hurtubise K. Cholecystocolonic fistula. Hawaii J Med Public Health. 2012;71(6):155-157.
- Chowbey PK, Bandyopadhyay SK, Sharma A, Khullar R, Soni V, Baijal M. Laparoscopic management of cholecystoenteric fistulas. J Laparoendosc Adv Surg Tech A. 2006;16(5):467-472. doi:10.1089/lap.2006.16.467