Peer Reviewed
Purpura, Arthralgia, and Acute Kidney Injury in a Patient With Sepsis
Answer: Leukocytoclastic Vasculitis (LCV)
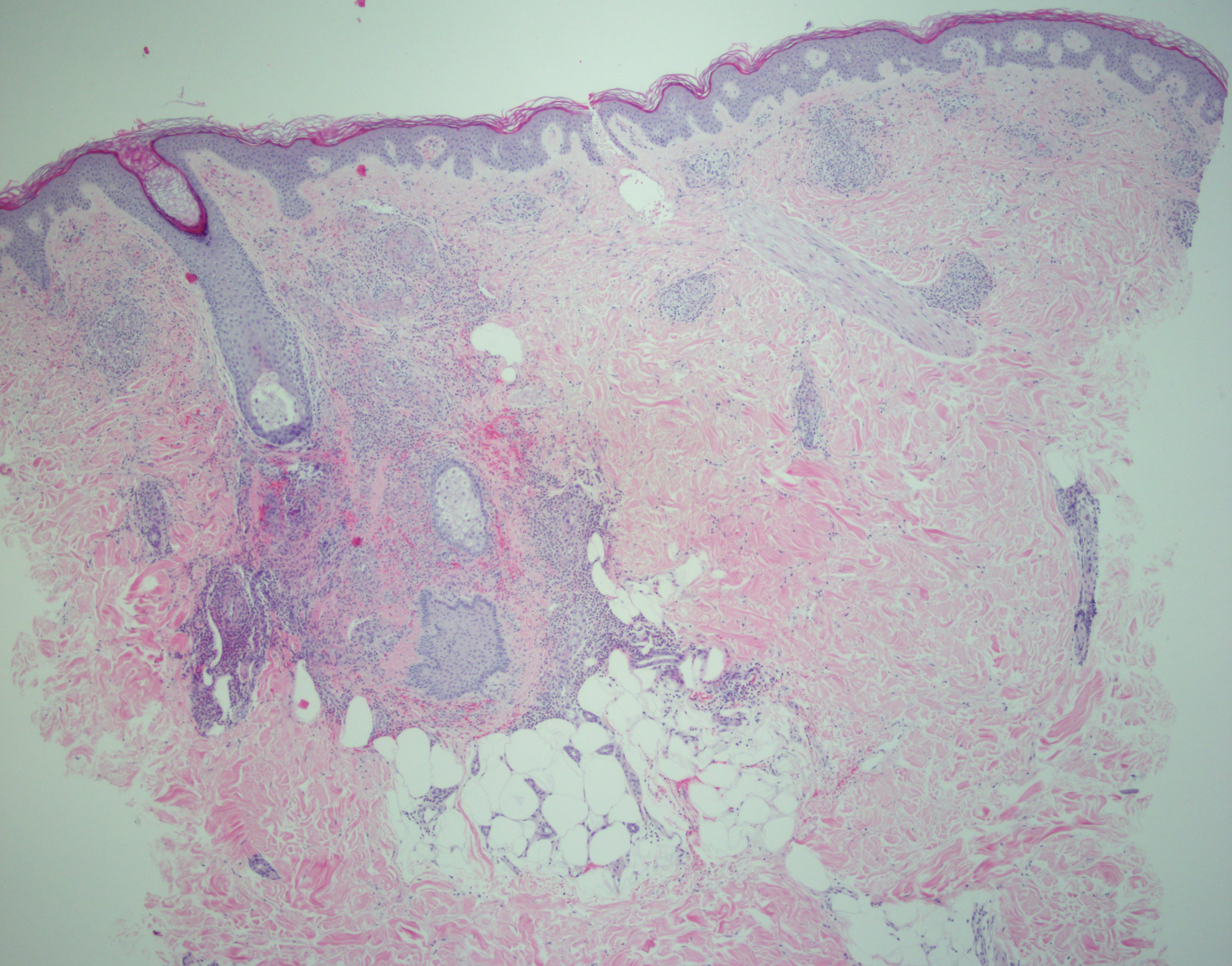
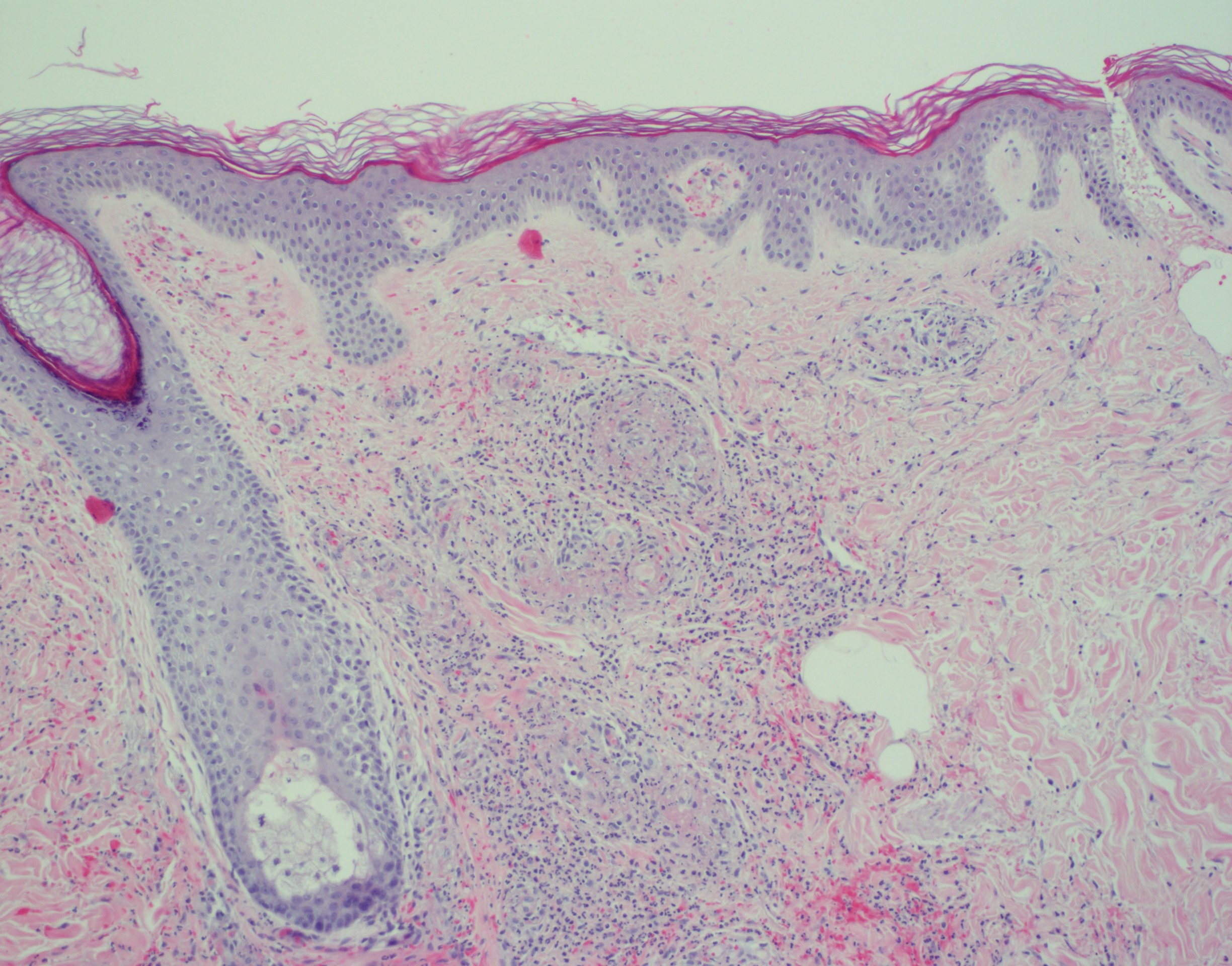
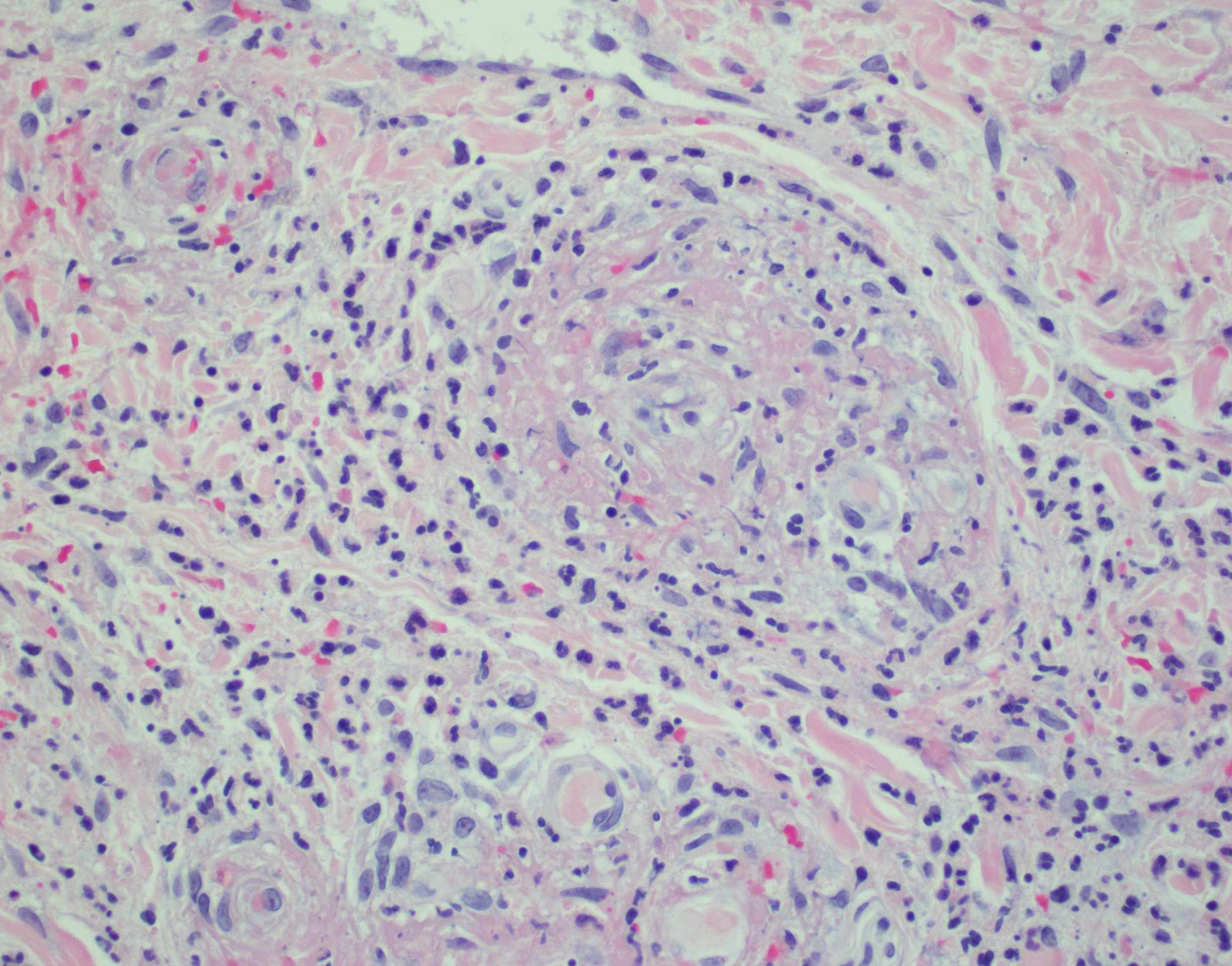
The rapid development of coalescing palpable purpura, acute kidney injury, and joint arthralgias subsequent to initiating a new medication strongly suggests a hypersensitivity vasculitis.1 Histopathologic study revealed neutrophilic vasculitis with red blood cell extravasation, perivascular and interstitial neutrophils, nuclear dust, and vascular damage with fibrin deposition (Figures 2-4). Under direct immunofluorescence, deposition of immunoglobulin G, immunoglobulin A, C3, immunoglobulin M, and fibrin were observed in the blood vessels and vessel walls. These findings confirmed the diagnosis of LCV.2

Figure 2. Section from a punch biopsy of skin lesions demonstrating neutrophilic vasculitis with erythrocyte extravasation, perivascular and interstitial neutrophils, nuclear dust, and vascular damage with fibrin deposition (hematoxylin-eosin; ×40 magnification).
Figure 3. Section from a punch biopsy of skin lesions demonstrating neutrophilic vasculitis with erythrocyte extravasation, perivascular and interstitial neutrophils, nuclear dust, and vascular damage with fibrin deposition (hematoxylin-eosin; ×100 magnification)
Figure 4. Section from a punch biopsy of skin lesions demonstrating neutrophilic vasculitis with erythrocyte extravasation, perivascular and interstitial neutrophils, nuclear dust, and vascular damage with fibrin deposition (hematoxylin-eosin; ×400 magnification).Fluoroquinolones are among the drugs known to induce vasculitis.3 Medication use also accounts for most cases of SJS and DRESS.4,5 However, SJS is more commonly associated with epidermal necrosis and involvement of 2 or more mucosal sites.4 DRESS usually appears several weeks after the first introduction of an offending medication.5 Eosinophilic granulomatosis with polyangiitis may present with cutaneous vasculitis and renal damage; lack of infiltrating eosinophils on skin biopsy demotes this diagnosis.6
The vasculitides are a heterogeneous group of diseases that are commonly grouped by the size of involved vessels, and LCV is the most common small vessel vasculitis. It involves the superficial vessels of the skin, whereas other vasculitides such as polyarteritis nodosa, nodular vasculitis, and giant cell arteritis affect deep muscular vessels found at the dermis-subcutis interface and within the subcutis.7 The skin is frequently involved in both localized and systemic presentations of vasculitis due to its large vascular bed, exposure to relatively colder temperatures, and the presence of stasis, especially in dependent areas.
Cutaneous vasculitis classically presents as palpable purpura but may exhibit a range of severity from simple erythematous lesions to necrosis, deep ulceration, and hemorrhagic blisters.2 Early lesions are largely asymptomatic, but as they mature may become pruritic and painful. Associated edema, especially in the lower extremities or dependent areas, may also occur. Vasculitis may be limited to the skin, or patients may exhibit systemic findings, and end-organ injury can arise secondary to ischemia or infarction.8 This may occur when the vessel wall damage causes hemorrhage and aneurysm formation or intimal hyperplasia leading to stenosis. Commonly affected sites include kidneys, heart, nervous system, gastrointestinal tract, lung, and joints.
LCV is a clinicopathologic diagnosis.9 Early inflammation of the small vessels is caused by a mixed infiltrate comprised mainly of neutrophils in addition to other mononuclear cells. When these leukocytes degenerate, in a process known as leukocytoclasis, the remaining perivascular nuclear debris is noted on histological study.10
It is unknown whether previous use of fluoroquinolones sensitizes a patient to subsequent exposures.11 Cutaneous vasculitis has been reported to occur in ciprofloxacin-naïve patients and in patients who had received ciprofloxacin previously without known reactions.3 This patient had used both oral ciprofloxacin and otic ofloxacin within the past 4 years with no noted reaction. A high index of suspicion is paramount, since drug hypersensitivity is not time- or dose-dependent.12 Objective scales exist to aid in clinical decision making.13
Failure to recognize drug-induced LCV can have dire consequences with regard to morbidity and mortality. Thus, initial management should include immediate cessation of the offending agent.9 A few anecdotal case reports advocate the use of corticosteroids for cutaneous LCV only in the setting of skin necrosis, usually made evident by hemorrhagic blisters or a gray appearance of the epidermis.14 Following removal of the offending drug, formal diagnostic workup should begin while monitoring for clinical change.
Outcome of the Case
Use of the Naranjo Adverse Drug Reaction Probability Scale indicated a probable relationship between the clinical findings and ciprofloxacin therapy in this patient.13 Ten days after discontinuing ciprofloxacin, the presented patient experienced a near-complete resolution of skin lesions with only mild postinflammatory hyperpigmentation remaining. Her acute kidney injury resolved over the following 2 weeks. She continued to experience wrist pain several months following exposure. Radiographic findings were unremarkable, and further workup is ongoing.
References:
- Carlson JA, Cavaliere LF, Grant-Kels JM. Cutaneous vasculitis: diagnosis and management. Clin Dermatol. 2006;24(5):414-429.
- Carlson JA. The histological assessment of cutaneous vasculitis. Histopathology. 2010;56(1):3-23.
- Lieu PK, Tok SC, Ismail NH, Chng HH. Ciprofloxacin-induced cutaneous vasculitis. Allergy. 1997;52(5):593-594.
- Miliszewski MA, Kirchhof MG, Sikora S, Papp A, Dutz JP. Stevens-Johnson syndrome and toxic epidermal necrolysis: an analysis of triggers and implications for improving prevention. Am J Med. 2016;129(11):1221-1225.
- Husain Z, Reddy BY, Schwartz RA. DRESS syndrome: Part I. Clinical perspectives. J Am Acad Dermatol. 2013;68(5):693.e1-693.e14.
- Mouthon L, Dunogue B, Guillevin L. Diagnosis and classification of eosinophilic granulomatosis with polyangiitis (formerly named Churg-Strauss syndrome). J Autoimmun. 2014;48-49:99-103.
- Fiorentino DF. Cutaneous vasculitis. J Am Acad Dermatol. 2003;48(3):311-340.
- Storsley L, Gerldenhuys L. Ciprofloxacin-induced ANCA-negative cutaneous and renal vasculitis—resolution with drug withdrawal. Nephrol Dial Transpl. 2007;22(2):660-661.
- Chen K-R, Carlson JA. Clinical approach to cutaneous vasculitis. Am J Clin Dermatol. 2008;9(2):71-92.
- Maunz G, Conzett T, Zimmerli W. Cutaneous vasculitis associated with fluoroquinolones. Infection. 2009;37(5):466-468.
- Blyth DM, Markelz E, Okulicz JF. Cutaneous leukocytoclastic vasculitis associated with levofloxacin therapy. Infect Dis Rep. 2012;4(1):e
- Mullick FG, McAllister HA Jr, Wagner BM, Fenoglio JJ Jr. Drug related vasculitis: clinicopathologic correlations in 30 patients. Hum Pathol. 1979;10(3):313-325.
- Naranjo CA, Busto U, Sellers EM, et al. A method for estimating the probability of adverse drug reactions. Clin Pharmacol Ther. 1981;30(2):239-245.
- Sunderkötter C, Bonsmann G, Sindrilaru A, Luger T. Management of leukocytoclastic vasculitis. J Dermatolog Treat. 2005;16(4):193-206.