
Peer Reviewed
Can You Identify the Cause of This Patient’s Chest Pain?
AUTHORS:
Michael Weipert, MD • Sean O’Mara, MDAFFILIATIONS:
US Navy Aerospace Medicine, Naval Hospital Pensacola, FloridaCITATION:
Weipert M, O’Mara S. Can you identify the cause of this patient’s chest pain? Consultant. 2020;60(12):15-17, 23. doi:10.25270/con.2020.06.00014Received February 19, 2020. Accepted May 11, 2020.
DISCLOSURES:
The authors report no relevant financial relationships.DISCLAIMER:
The views expressed in this article are those of the authors and do not necessarily reflect the official position of the institution, the Department of the Navy, the Department of Defense, or the United States Government.CORRESPONDENCE:
Michael Weipert, MD, Naval Hospital Pensacola, 6000 US-98, Pensacola, FL 32512 (michael.j.weipert.mil@mail.mil)A 39-year-old previously healthy woman presented to an urgent care clinic with chest pain that had been present for the past 4 days. She reported that the pain, which she rated as 7 on a 10-point scale, had been steady and had not resolved despite her having taken over-the-counter nonsteroidal anti-inflammatory drugs.
She stated that she felt as if her chest was being crushed, and she also noted that it hurt when she took a deep breath. She also reported having musculoskeletal pain in her right shoulder, which she said may have been related to a recent intense workout, but she denied any known mechanism of injury. She stated that she believed her chest pain to be unrelated to her shoulder pain. She noted that the chest pain was worse at night, especially when lying down, and subsided while she was eating.
She had no personal or family history of cardiac disease, and her medical history was significant only for acid reflux. Her social history was negative for tobacco use, and her employment consisted primarily of desk work.
Her vital signs were normal, with an oxygen saturation at 99% on room air. The patient was thin, well dressed, and in minimal discomfort. Physical examination findings were unremarkable, with normal cardiac and chest sounds present. An electrocardiogram (ECG), chest radiographs, a complete blood cell count (CBC), a basic metabolic panel (BMP), and tests for troponin, creatine kinase–MB fraction (CK-MB), and D-dimer levels were ordered. The ECG showed normal sinus rhythm, regular rate, normal cardiac axis, and no ST-segment elevations (Figure 1).
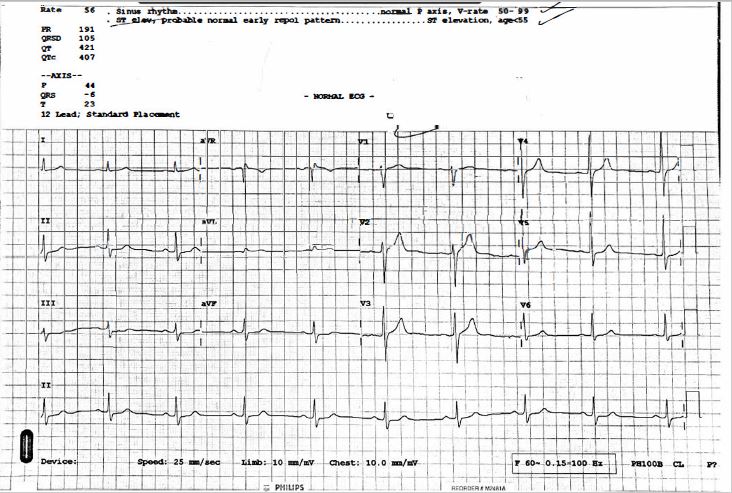
Figure 1. ECG of a 39-year-old woman with a 4-day history of chest pain.The CBC, BMP, and troponin, CK-MB and D-dimer levels were all within normal levels. She was given a gastrointestinal cocktail of aluminum hydroxide and magnesium hydroxide suspension and viscous lidocaine; after 10 minutes, and she stated that her chest pain had improved.
The chest radiographs returned, the findings of which are shown in Figure 2.

Figure 2. Chest radiograph of a 39-year-old woman with a 4-day history of chest pain.