
Clinical Consequences of Sun Exposure

Favre-Racouchot Nodular Elastosis
A 69-year-old woman, who was being seen regularly for treatment of psoriasis, was noted to have numerous open comedones on the sides of her face in association with photodamaged skin.
This is Favre-Racouchot nodular elastosis (or nodular elastoidosis with cysts and comedones), a condition classified in the group known as the solar elastotic syndromes; they are characterized microscopically by the accumulation of degenerative material that stains with elastic tissue stains.
Favre-Racouchot syndrome, which is more prevalent in men, typically affects the periorbital and malar skin but may also occur at other sites of photodamage, such as the nose, neck, and retroauricular area. Initially, enlarged pilosebaceous orifices filled with keratinous debris appear on a background of photodamaged skin. In some advanced cases, cystic nodules develop that may coalesce into thickened, yellowish plaques containing large comedones. The condition is thought to result from weakening of the supporting stroma surrounding pilosebaceous units secondary to photodamage.
(Case and photograph courtesy of Drs Eric J. Lewis and Charles E. Crutchfield III.)
FOR MORE INFORMATION:
- Calderone DC, Fenske NA. The clinical spectrum of actinic elastosis. J Am Acad Dermatol. 1995;32:1016-1024.
- Fenske NA, Lober CW. Aging and its effects on the skin. In: Moschella SL, Hurley HJ, eds. Dermatology. 3rd ed. Philadelphia: WB Saunders Company; 1992:107-122.
- Lyon NB, Fitzpatrick TB. Geriatric dermatology. In: Fitzpatrick TB, Eisen AZ, Wolff K, et al, eds. Dermatology in General Medicine. New York: McGraw-Hill; 1993:2961-2979.

Actinic Keratoses
The possibility that the lesion on his upper right arm (A) might be cancerous prompted a 77-year-old man to seek medical care. The patient had had a squamous cell carcinoma and 2 basal cell carcinomas removed during the past 5 years.
This lesion was excised under local anesthesia. It proved to be an actinic keratosis—a common, sun-induced, premalignant lesion. Often yellow-brown or red, solar keratoses frequently are seen in elderly persons who have a history of habitual sun exposure. The keratoses are rough, scaly, and round or oval. Single or multiple keratoses may arise.
Figure B shows a lesion that developed on a 67-year-old man’s forehead. This eruption measured 0.8 × 0.8 cm; it was fleshy and well-demarcated. Unusual wart-like
cylindrical projections complicated the diagnosis.
The lesion was completely excised; histologic examination disclosed hypertrophic actinic keratosis. The lesion was benign but premalignant. A small percentage of actinic keratoses may progress to squamous cell carcinoma.
A 72-year-old woman with long-term sun exposure had a crusted, nodular, erythematous plaque on the distal extensor surface of the left forearm, just above the wrist (C). The gradually enlarging lesion had been present for years; it was excised in the office.
Histologic examination disclosed inflamed actinic keratosis with severe Bowenoid dysplasia. The term “Bowenoid” indicates a similarity to Bowen’s disease, or squamous cell carcinoma in situ.
In addition to surgical excision, actinic keratoses may be treated with cryotherapy, tretinoin, acid peels, and topical 5-fluorouracil or masoprocol. Strongly encourage the use of sunscreens.
(Cases and photographs courtesy of Dr Robert P. Blereau.)

Phytophotodermatitis
A 23-year-old woman presented with an odd, circular pattern imprinted on her upper right back and linear markings on her lower back. She explained that recently her husband had placed 2 iced beer mugs with wedges of lime on their rims on her back as she lay sunbathing. The double-circle and striated designs on her skin were not painful, just faintly pruritic and unsightly.
The history coupled with the bizarre design led to the diagnosis of phytophotodermatitis—hyperpigmentation caused by application of photosensitizing plant material followed by exposure to light. Here, the combination of lime juice and sunlight produced a phytophotoallergic rash that left the pattern of postinflammatory hyperpigmentation on the patient’s dark skin. The configuration of the beer mugs is evident; the lower back features discoloration caused by pooling and dripping lime juice.
Other substances that induce phytophotodermatitis include celery and carrot greens; phytophotodermatitis has been described in persons who harvest these vegetables. Oil of bergamot, bitter orange, and lemon may cause this condition as well.
Because of the patient’s dark skin, the postinflammatory hyperpigmentation took several months to resolve completely. Topical corticosteroids may be used to ease the pruritus and inflammation; azelaic acid can help reduce postinflammatory hyperpigmentation.
(Case and photograph courtesy of Joe Monroe, PA-C.)
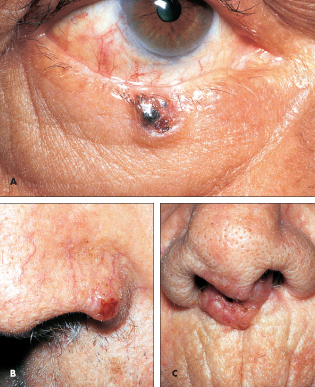
Basal Cell Carcinoma
Basal cell carcinomas are the most common skin malignancy. Most frequently, their development is attributable to sun exposure; more than 90% of these lesions arise on sun-
exposed skin of the head and neck. These slow-growing malignancies rarely metastasize; the cure rate is nearly 100%.
Basal cell carcinomas arise most often in men older than 50 years. The pigmented basal cell carcinoma on a 64-year-old man’s lower eyelid (A) had been present for 4 years. An excellent cosmetic result was achieved by shave excision of the lesion.
Complete excision was used to treat the nodular, centrally pigmented basal cell carcinoma that arose on a 74-year-old man’s left nostril (B).
Although these lesions are typically seen in men, women are not immune. An 84-year-old woman had a basal cell carcinoma on her upper lip (C) of several years’ duration. It had begun to grow into the columella. The patient refused surgical excision.
(Cases and photographs courtesy of Dr Robert P. Blereau.)

Lentigo
A 1.5-cm, flat, brown, pigmented macule is located lateral to a 40-year-old woman’s right eye. The lesion had been present for at least 2 years; it recently darkened.
Because of the color change, a biopsy of the macule was performed. Microscopic examination of the specimen revealed a benign lesion with orthokeratosis, some saw-toothing of epidermal retia with a slight increase of basilar melanogenesis. The diagnosis of lentigo was made. Reassuring the patient was the only therapy necessary.
Lentigines, or liver spots, arise on sun-exposed areas, usually the face, arms, and hands. The lesions are generally 0.2 to 2.0 cm in diameter and increase in number with advancing age.
A change in a lentigo may signal malignant transformation and the need for microscopic examination. Perform a biopsy to rule out melanoma when a lentigo thickens, its pigmentation darkens, or the borders become irregular.
When the patient requests removal of the lentigo, consider excision, cryotherapy, or topical tretinoin.
(Case and photograph courtesy of Dr Robert P. Blereau.)
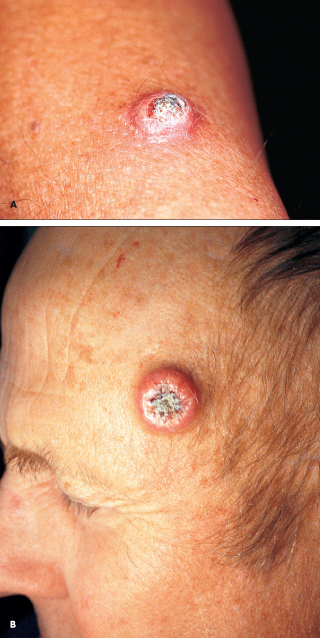
Keratoacanthoma
A 66-year-old man reported that the “growth on my arm seemed to come on over a few weeks (A).” Rapid growth is characteristic of a keratoacanthoma, an epithelial neoplasm.
The classic keratoacanthoma is a sharply marginated, dome-shaped nodule with a keratin-filled core. Typically, these lesions arise on sun-damaged, hair-bearing areas during mid to late life. Men are affected twice as often as women.
Figure B shows a keratoacanthoma on the temple of a 60-year-old man. The nodule, which has a characteristic well-defined keratotic core, grew to this size within 8 weeks. The patient’s history included chronic, poorly tolerated sun exposure and recent corticosteroid therapy for temporal arteritis. Keratoacanthomas are seen frequently in immunosuppressed persons.
A keratoacanthoma can grow to a diameter of 2.5 cm in 2 months and maintain that size for another 2 to 8 weeks. During the next 2 to 8 weeks, the nodule may undergo spontaneous involution and leave an atrophic scar at the original site.
Because keratoacanthoma is a subtype of squamous cell carcinoma, do not wait for the lesion to involute spontaneously. Prompt removal and pathologic examination of the lesion are recommended.
(Case and photograph A courtesy of Drs Charles E. Crutchfield III, Eric J. Lewis, and Humberto Gallego. Case and photograph B courtesy of Joe Monroe, PA-C.)

Solar Elastosis
Skin changes on the forehead and scalp prompted an 81-year-old man to seek medical consultation. His history included years of working outdoors without wearing a hat and many episodes of sunburn.
The skin of the scalp, forehead and, particularly, the temples appeared whitish and thickened. The skin of the lower face and neck was weathered and dotted with numerous actinic keratoses and telangiectases.
This patient’s skin exhibits signs of dermatoheliosis, or chronic sun damage, which leads to photoaging. The skin changes on the patient’s forehead and scalp represent solar elastosis, which is typically seen in dermatoheliosis. Solar elastosis is brought about by basophilic degeneration of the upper reticular layer. Swelling, coarsening, and late homogenization of connective tissue fibers in the upper dermis are associated with the loss of skin elasticity.
Underscore the need to continue to limit sun exposure and to use solar barriers. Schedule regular follow-up visits for your patients with dermatoheliosis; they are prime candidates for sun-induced skin cancers.
(Case and photograph courtesy of Joe Monroe, PA-C.)