
Peer Reviewed
Proteus Syndrome in a Young Adolescent
AFFILIATIONS:
1Medical Student, University College Dublin, Dublin, Ireland
2Resident Physician, Psychiatry Department, University of Chicago, Chicago, IL
3Professor Emeritus, McGovern Medical School, Houston, TX
CITATION:
Matthews M, Rosas L, Mazur L. Proteus syndrome in a young adolescent. Consultant. 2022;62(9):e22-e24. doi:10.25270/con.2022.03.00004
Received October 22, 2021; accepted November 8, 2021. Published online May 23, 2022.
DISCLOSURES:
The authors report no relevant financial relationships. Authors report that informed consent was
obtained for publication of the images used herein.
CORRESPONDENCE:
Miriam Matthews, University College Dublin, Belfield, Dublin 4, Ireland (mimymatthews@gmail.com)
Abstract
Proteus syndrome (PS) is a rare, progressive, asymmetric overgrowth syndrome that presents with symptoms of varying severity. This case report presents a 13-year-old boy with progressive enlargement of the left leg that was initially mistaken for filariasis. PS most commonly affects the limbs and occasionally presents with hamartomas and vascular malformations. Due to the progressive nature and risk of complications, such as limb length discrepancy, deep venous thromboses, skin ulcerations, and malignant neoplasms, PS should be considered in a differential diagnosis with other overgrowth syndromes.
Key words: Proteus syndrome, overgrowth syndrome, hamartomas, vascular malformation
On a medical mission trip to Tumbes, Peru, a 13-year-old boy presented with enlargement of his left leg. The father stated that his son’s leg had been progressively enlarging since early infancy. He said numerous treatments for parasitic illnesses had not helped. The family history was negative for anyone with similar findings.
The boy’s physical examination was remarkable for a body mass index greater than 95% for his age, enlargement of his left leg with areas of cratered scars below the knee, and a leg-length discrepancy (Figures 1 and 2).


No other areas of the body were affected. He had no macrocephaly, ocular anomalies, hemangiomas, nevi, or scoliosis.
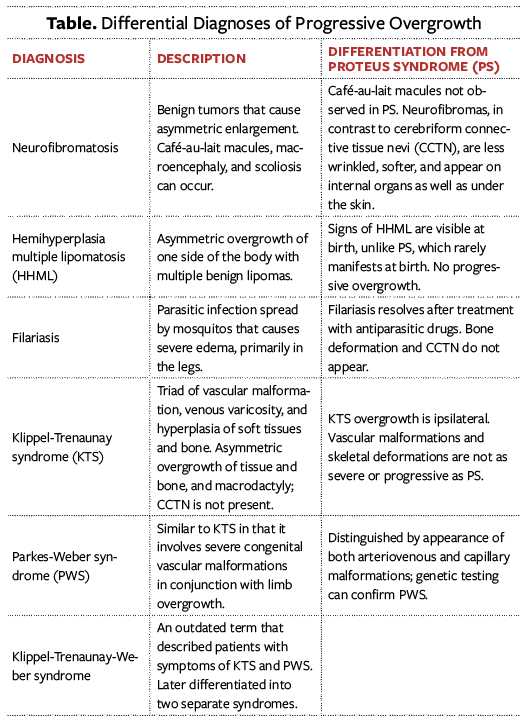
The differential diagnoses included hemihyperplasia, Proteus syndrome (PS), and Klippel-Trenaunay syndrome (KTS) (Table). Because of the progressive enlargement of the leg and lack of vascular markings, PS was considered the most likely diagnosis.1
Discussion
A rare genetic disorder, PS manifests with progressive, asymmetric overgrowth of the limbs with occasional hamartomas and vascular malformations.1,2 It has an estimated prevalence between 1:1,000,000 and 1:10,000,000.1 It was named by Hans-Rudolf Wiedemann in 1983 after the Greek shapeshifter god Proteus, and it is thought that Joseph Merrick (the so-called “Elephant Man”) had PS.3 Patients with PS typically have no anomalies at birth but develop asymmetric and irregular overgrowth between 6 and 18 months of age.1 The overgrowth continues until adolescence and then plateaus.1,4 The limbs are most commonly affected but the location and severity of the deformations may vary.5
PS is thought to be caused by somatic mosaicism in the AKT1 gene on chromosome 14.1,2 It belongs to a class of genes known as oncogenes and provides instructions for making AKT1 kinase. The protein is found in various cells throughout the body and plays a critical role in signaling pathways. Nonmosaic mutations are thought to be lethal but a duplication of the AKT1 gene causing PS has been reported.1,6 As PS is not genetically inherited, offspring are not at increased risk and prenatal testing is not necessary.1 However, few patients with PS have reproduced.1 The diagnosis is usually based on clinical findings but can be confirmed with testing for AKT1 mutations.1 However, as mosaicism may be limited to certain tissues, testing is difficult.6 Unfortunately, imaging and testing for our patient were not possible because of the remote location.
Complications vary in severity and may include dermatologic malformations, central nervous system manifestations, pulmonary emboli, skeletal overgrowth, and deep venous thromboses (DVT).1 Although patients may have cutaneous capillary malformations, venous and arterial malformations are less common.5
One pathognomonic sign is the presence of cerebriform connective tissue nevi (CCTN) that most commonly appear on the palms and soles.2,5 The lesions have not been observed at birth but develop slowly during adolescence.5 This brain-groove pattern thickens over time and complicates hygiene in the affected areas.2,5 Their presence also distinguishes PS from KTS.4 Linear epidermal nevi are also a common manifestation and darken over time.1,5
Central nervous system manifestations occur in 40% of patients, mental deficiency in 30%, and epilepsy in 10%.
Hydrocephalus, hemimegalencephaly, Dandy-Walker malformations, polymicrogyria, heterotopia, and various cysts have also been reported.4 Benign and malignant neoplasms such as ovarian cystadenomas, parotid adenomas, mesotheliomas, and overgrowth of the spleen, liver, and lungs can also occur.1,2 Facial phenotypes can include dolichocephaly, down-slanting palpebral fissures, low nasal bridge, widened nares, long face, and an open mouth at rest.4,5 Craniofacial abnormalities such as hyperostosis and unilateral condylar hyperplasia also occur.4 Bony overgrowths can calcify and further distort and restrict movement at affected joints.1.5 Leg-length discrepancies of 20 cm, scoliotic curves of over 90 degrees, and bone age retardation are also possible.1,5,7 Dysregulation of adipose tissue can result in both lipoatrophy and overgrowth.2 Lipoatrophy commonly occurs in the chest while fatty overgrowth presents in the abdomen and extremities.5
Treatment options address complications as they arise. Guidelines recommend a skeletal survey, chest computed tomography scans, and abdominal magnetic resonance imaging to identify pulmonary lesions and abdominal lipomas.4 Multiple orthopedic procedures may be necessary for skeletal overgrowth. Reduction osteotomies (selected removal of bone tissue to reduce overgrowth) and epiphysiodesis (ablation of epiphyses to arrest growth) can be beneficial. Shoe lifts and custom footwear may help with minor leg-length discrepancies. Spinal fusion for vertebral overgrowth and surgical correction of
scoliosis may arrest kyphoscoliosis and prevent pulmonary compromise.1,4
If CCTN develops, a dermatologist can help manage hygiene and pressure ulcerations.1 Pedorthic (podiatric services) and surgical intervention to remove plantar CCTN may be required.1 Surgical treatment of adipose overgrowth may be difficult because of diffuse overgrowth.1
Patients of all ages are at high risk for pulmonary emboli and DVT, especially with surgical interventions. Therefore, perioperative anticoagulant prophylaxis is recommended.5 Procoagulants or medications that promote growth (such as steroids) should be avoided because of the risk of DVT.
When possible, consultations with genetics, pediatrics, dermatology, and orthopedics are helpful. Patients and caregivers may feel isolated because of progressive disfiguring, so all may benefit from referral to behavioral health care providers and family support groups.4 The life expectancy for PS depends on the severity of the complications but ranges between 9 months and 29 years.2 The father was informed of the possible complications and was given a guarded prognosis and life expectancy of a patient with PS.
1. Biesecker LG, Sapp JC. Proteus syndrome. In: Adam MP, Ardinger HH, Pagon RA, et al, eds. GeneReviews (internet). University of Washington, Seattle; 2019.
2. Rocha R de CC, Estrella MPS, do Amaral DM, Barbosa AM, de Abreu MAMM. Proteus syndrome. An Bras Dermatol. 2017;92(5):717-720. doi:10.1590/abd1806-4841.20174496
3. Tibbles JA, Cohen MM. The Proteus syndrome: the Elephant Man diagnosed. Br Med J (Clin Res Ed). 1986;293(6548):683-685. doi:10.1136/bmj.293.6548.683
4. Cohen MM. Proteus syndrome: an update. Am J Med Genet C Semin Med Genet. 2005;137C(1):38-52. doi:10.1002/ajmg.c.30063
5. Biesecker L. The challenges of Proteus syndrome: diagnosis and management. Eur J Hum Genet. 2006;14(11):1151-1157. doi:10.1038/sj.ejhg.5201638
6. AlAnzi T, Al-Mashharawi E, Alhashem A. Proteus syndrome caused by novel somatic AKT1 duplication. Saudi Med J. 2021;42(1):95-99. doi:10.15537/smj.2021.1.25618
7. Wiedemann HR, Burgio GR, Aldenhoff P, Kunze J, Kaufmann HJ, Schirg E. The proteus syndrome. Eur J Pediatr. 1983;140(1):5-12. doi:10.1007/BF00661895