
Peer Reviewed
Subclinical Pyelonephritis Presenting as Relapsing Fever: A Prodrome in the Development of Chronic Pyelonephritis
AUTHORS:
Paul Shiu, DO1 • Anil Harrison, MD2,3 • Priya Nand, MD4
AFFILIATIONS:
1Internal Medicine Resident, St. Joseph’s Medical Center, Stockton, California
2Associate Program Director, Internal Medicine Residency Program, St. Joseph’s Medical center, Stockton, California
3Medical Director, Touro University Medical Group, Stockton, California
4Infectious Disease Physician, Touro University Medical Group, Stockton, California
CITATION:
Shiu P, Harrison A, Nand P. Subclinical pyelonephritis presenting as relapsing fever: a prodrome in the development of chronic pyelonephritis. Consultant. 2022;62(6);e8-e9. doi:10.25270/con.2021.08.00006
Received February 6, 2021. Accepted April 27, 2021. Published online August 12, 2021
DISCLOSURES:
The authors report no relevant financial relationships.
CORRESPONDENCE:
Paul Shiu, DO, St. Joseph’s Medical Center, 1800 North California Street, Stockton, CA 95204 (Paul.Shiu@DignityHealth.org)
A 36-year-old man presented for evaluation of relapsing fevers. He reported fevers as high as 40 °C and has had 6 such episodes in the past 6 months that have lasted between 2 to 14 days. During these episodes, he also reported shaking chills, myalgias, and arthralgias as well as brief and intermittent episodes of cough, diarrhea, and headache. He denied weight loss but reported night sweats unrelated to fever. A review of all other systems was unremarkable.
History. The patient was of Indian descent, born on the Fiji Islands, and has been living in California for more than 20 years. He is a building contractor by occupation and works in unsanitary crawl spaces. He had no known insect or rodent bites. He reported practicing safe sex.
Except for taking acetaminophen and low-dose ibuprofen for fever and constitutional symptoms, he denied taking any other medications or using recreational drugs. He denied exposure to ticks, livestock, birds, and domesticated pets. His vaccinations are up to date including the Bacillus Calmette-Guérin (BCG) vaccination, which he received as a child.
A few months after his first febrile episode, he received a diagnosis of acute otitis media and was prescribed a 10-day course of amoxicillin-clavulanate. However, the fevers persisted. Six months prior to presenting at our clinic, he had traveled to Fiji where he had drunk water from a stream, the ocean, and a river and consumed unpasteurized milk and uncooked foods.
Diagnostic testing. Upon presentation, our patient’s vital signs and physical examination were within normal limits. Laboratory workup, serology and immunology studies, and a nucleic acid amplification test were performed, and cultures were collected. Results were unremarkable except for an elevated level of C-reactive protein (73.7 mg/dL; reference range, < 8 mg/dL), an elevated level of leukocytes in the urine (10-20/hpf; reference range, < 5/hpf), and a positive leukocyte esterase screen on urinalysis.
A computed tomography (CT) scan of the chest and abdomen was remarkable for small calculi in both upper poles of the kidneys, findings suggestive of pyelonephritis involving the right kidney (Figure). No organisms were isolated from the urine sample, but our clinical suspicion for pyelonephritis was high. The patient was prescribed a 10-day course of oral ciprofloxacin, 500 mg, twice a day.
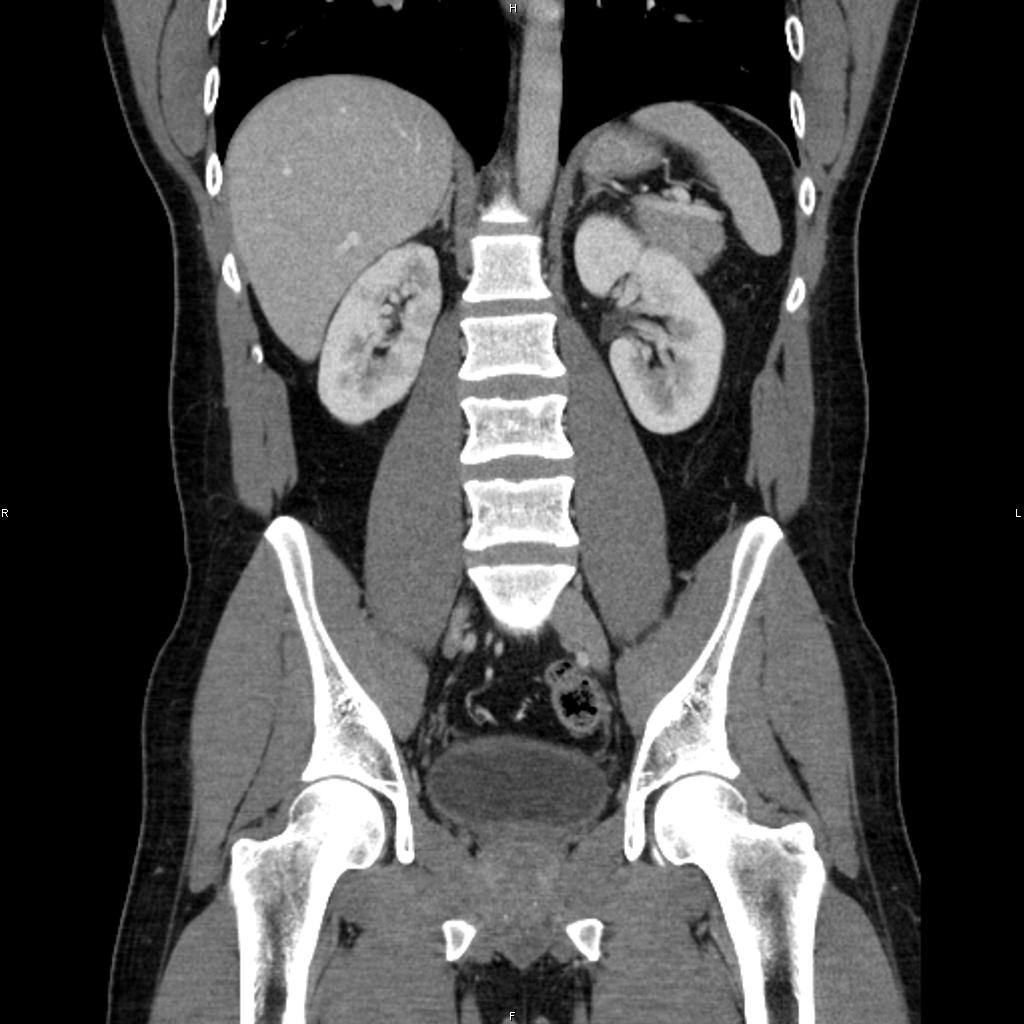
Figure. The overall size of the right kidney is slightly smaller than the left. There is also cortical irregularity to the upper pole, which can be congenital but can also be scarring from prior pyelonephritis or infarcts. Other supportive radiographic features for chronic pyelonephritis include calyceal clubbing and renal asymmetry or atrophy accompanied by cortical thinning.
Discussion. Relapsing fevers are defined as recurrent fevers that are sudden in onset and are punctuated by intervening afebrile periods. The usual causes are arthropod-borne infections such as tick-borne relapsing fever and louse-borne relapsing fever.1,2 Malaria, babesiosis, ehrlichiosis and anaplasmosis, typhoid, tularemia, brucellosis, leptospirosis, rickettsiosis, dengue, and autoinflammatory illness also need to be considered. One of the infrequent and lesser-known etiologies is “inapparent” or “subclinical” pyelonephritis, which presents with episodic symptomatic phases that can persist or smolder as symptomless bacteriuria. This can eventually lead to chronic pyelonephritis, a disease that was once promulgated as the most common cause of kidney failure.3-5 Chronic pyelonephritis is a complex renal disorder characterized by chronic tubulointerstitial inflammation and deep segmental cortical renal scarring and clubbing of the pelvic calyces as the papillae retract into the scar. It is an important cause of end-stage renal disease (ESRD). Here we present a case of subclinical infection that resulted in inapparent pyelonephritis.
Our patient with recurring fevers had no urinary symptoms and a physical examination within normal limits. The exhaustive workup revealed a significantly elevated C-reactive protein level, sterile pyuria (negative for bacteria, acid-fast bacillus, and fungi), and renal micro calculi with changes suggestive of pyelonephritis involving the right kidney on contrast-enhanced CT scan of the chest and abdomen.
Patient outcome. Following a 10-day course of ciprofloxacin, his fevers had resolved, and the urine abnormalities had normalized. Invasive workup such as renal biopsy, excretory urography scan, and testing for uromodulin were not pursued, because his CT scan did not demonstrate any asymmetry or structural irregularities.
The authors feel that a progression from “inapparent” or “subclinical” pyelonephritis to a state of chronic pyelonephritis, perhaps progressing to ESRD, has possibly been averted. The patient has not had any further bouts of relapsing fevers or any constitutional symptoms for more than 7 months. The authors’ plan is to follow up about the patient’s serum creatinine level, glomerular filtration rate, and urinalysis biannually.
References
1. Barbour AG. Relapsing fever. In: Goodman JL, Dennis DT, Sonenshine DE, eds. Tick-Borne Diseases of Humans. American Society for Microbiology Press; 2005.
2. Barbour AG, Hayes SF. Biology of Borrelia species. Microbiol Rev. 1986;50(4):381-400. https://doi.org/10.1128/mr.50.4.381-400.1986
3. The role of asymptomatic bacteriuria in the pathogenesis of pyelonephritis. In: Quinn EL, Kass EH. Biology of Pyelonephritis. Little, Brown & Company; 1960.
4. Sanford JP. Inapparent pyelonephritis; the missing link. J Am Med Assoc. 1959;169(15):1711-1714. https://doi.org/10.1001/jama.1959.03000320013003
5. Gall EA. Pyelonephritis. Bull N Y Acad Med. 1961;37(6):367-382. http://www.ncbi.nlm.nih.gov/pmc/articles/pmc1804682/